A synthesis of some of the important information I have seen to date relating to FTO and bisantrene.
This research is my own and is intended to improve the knowledge of everyday investors, like myself. There may be mistakes in the my understanding of the science, although I have done my best to understand it and explain it from a laymans perspective.
If there is information that you think is important that is missing or could be improved upon, feel free to let me know and I'll include it.
This is not financial advice.2.0 Pillar 1 - FTO
The FTO protein is known as an ‘eraser’ for its role in DNA methylation, which is the removal of a methyl group (CH3) from RNA (Figure 1). The activity of the FTO molecule has downstream consequences for the production of proteins; where high activity of FTO decreases protein production due to a reduction of ‘active’ genes. FTO proteins are found throughout the body and have been extensively linked to obesity and cancer. In fact, FTO is significantly related to multiple biological functions of cancers, including cell cycle, tumor growth, proliferation, survival, migration, invasion, stem cell maintenance, and self-renewal. The majority of FTO mechanisms play critical roles in cancer tumorigenesis (tumour growth). For the purpose of this review, I will only focus on the relationship between FTO and cancer.
https://www.frontiersin.org/articles/10.3389/fendo.2018.00396/full
Figure 1: Image describing the pathways of methylation and demethylation.
RACs focus is described in the image below.
2.1 City of Hope paper
(https://www.researchgate.net/publication/342113813_Targeting_FTO_Suppresses_Cancer_Stem_Cell_Maintenance_and_Immune_Evasion)
The City of Hope (COH) paper is really where the story begins. As I write this synthesis, I’m still amazed by how amazing these findings were and how they changed the direction of RAC indefinitely. The story began with an inquiry into the National Cancer Institute Developmental Therapeutics Program (NCI DTP) library of 260,000 compounds. The City of Hope (COH) researchers requested the top 370 candidate compounds that showed the greatest scores based on their docking to FTO’s catalytic pocket. Assessment of their leukemic effects indicated the top 20 (Figure 2), where the inhibitory effects on FTO identified three compounds. The most clinically viable option was Bisantrene.
Key highlights from the study included:
Identification of potent FTO inhibitor with IC50 values in the low nanomolar range
KD of FTO or pharmacological inhibition of FTO suppresses LSC/LIC self-renewal
Targeting FTO suppresses immune checkpoint gene expression and immune evasion
Targeting FTO by potent inhibitors holds therapeutic promise against various cancers
Below is a short summary of the data taken from the study as well as some figures that add significant value to Bisantrene, referred to as CS1 throughout the paper. Also, you may see CS2 mentioned a lot, but there are clinical issues with this drug - inconsistencies are seen in performance in the clinic and as such, is not viable outside the clinic.
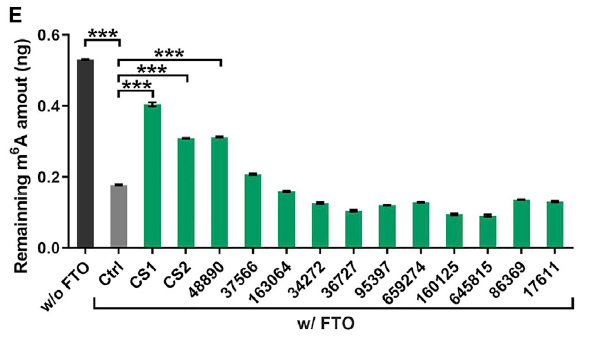
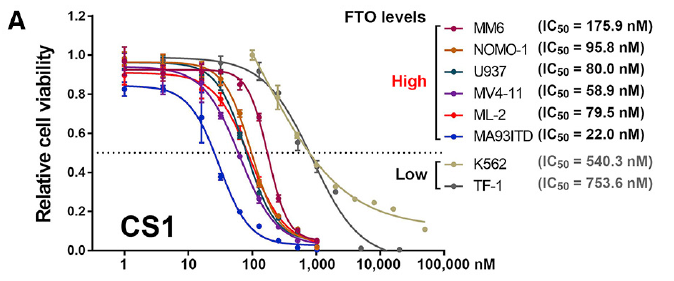
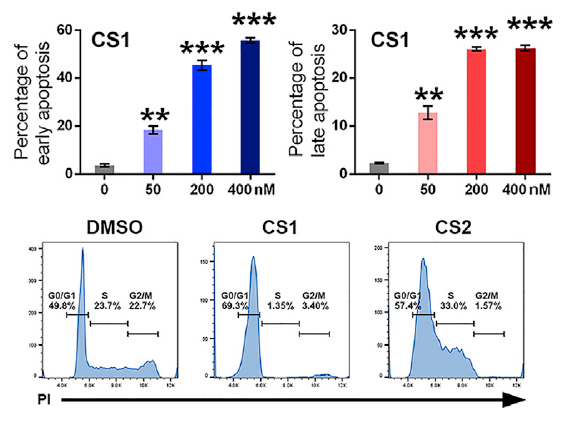
Briefly put, bisantrene is a one out of 260,000 drugs which selectively binds and occupies the catalytic pocket of FTO, blocking m6A-modified oligos from entering. This inhibits FTO’s demethylase activity and its binding with the target RNA transcripts. Bisantrene displayed the highest efficacy in inhibiting AML cell viability, with IC50 values 10 to 30-fold lower than other known FTO inhibitors (Figure 3). The effects of FTO knockdown (gene manipulation artificially decreasing FTO concentration) were consistent with Bisantrene’s pharmacological inhibition on AML cell viability and differentiation and on leukemia stem/Initiating cell self-renewal (Figure 4). This upregulation of apoptosis (cell death) was due to bisantrene modulating the signal pathways of FTO and changing the molecules normally produced. Micelles packaged bisantrene demonstrated significant anti-leukemic and anti-AML activity, suggesting Bisantrene would be effective in refractory AML (which it already is).
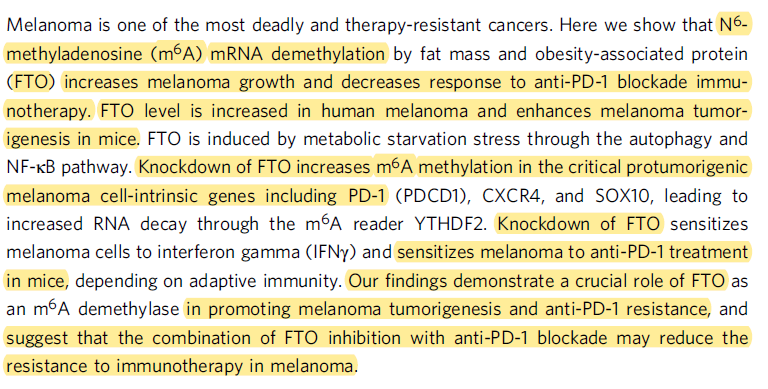
The study also showed that the FTO/m6A axis regulates immune checkpoint gene expression, which is important as upregulation of immune checkpoint genes, such as PD-1, PD-L1, and PD-L2, have been assumed to contribute to hypomethylating agent (HMA; a drug that inhibits DNA methylation)-induced drug resistance in treated patients. The author writes - “FTO inhibition significantly inhibited the expression of PD-L1 and PD-L2 in human AML cells with or without DAC treatment”. This is a fundamental aspect of the study and creates significant value for bisantrene, as Keytruda, a PD-1 inhibitor, is expected to reach USD ~25B in sales by 2025 and Bisantrene may make it more effective. Another checkpoint inhibitor LILRB4 was significantly downregulated upon inhibition of FTO by bisantrene, indicating that bisantrene could also be effective in AML cells. Targeting FTO with bisantrene also sensitized AML cells to T cell cytotoxicity and overcame HMA-induced immune evasion (Figure 5). And finally, the conclusion taken from the paper in Figure 6.
Figure 2: Effects of top 20 compounds on the enzymatic activity of FTO. Bisantrene (CS1) identified as the highest ranking.
Figure 3: Relative cell viability after exposure to Bisantrene (CS1).
Figure 4: Percentage of early apoptosis (top left), late apoptosis (top right), and effects of CS1 on cell-cycle distribution (note the efficacy compared to CS2).
Figure 5: (B-E) Effect of CS1 (B) and CS2 (D) on the sensitivity of human AML cells to the cytotoxicity of T cells in vitro.
Figure 6: City of Hope papers concluding statements.
Finally, I would like to make the point that following the results of this paper, the researchers at City of Hope investigated the patents surrounding bisantrene and unfortunately for them, realised that they were held securely and comprehensively by RAC, and in effect, its shareholders.
2.2 Cancer indications
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7751723/pdf/ott-13-12845.pdf).
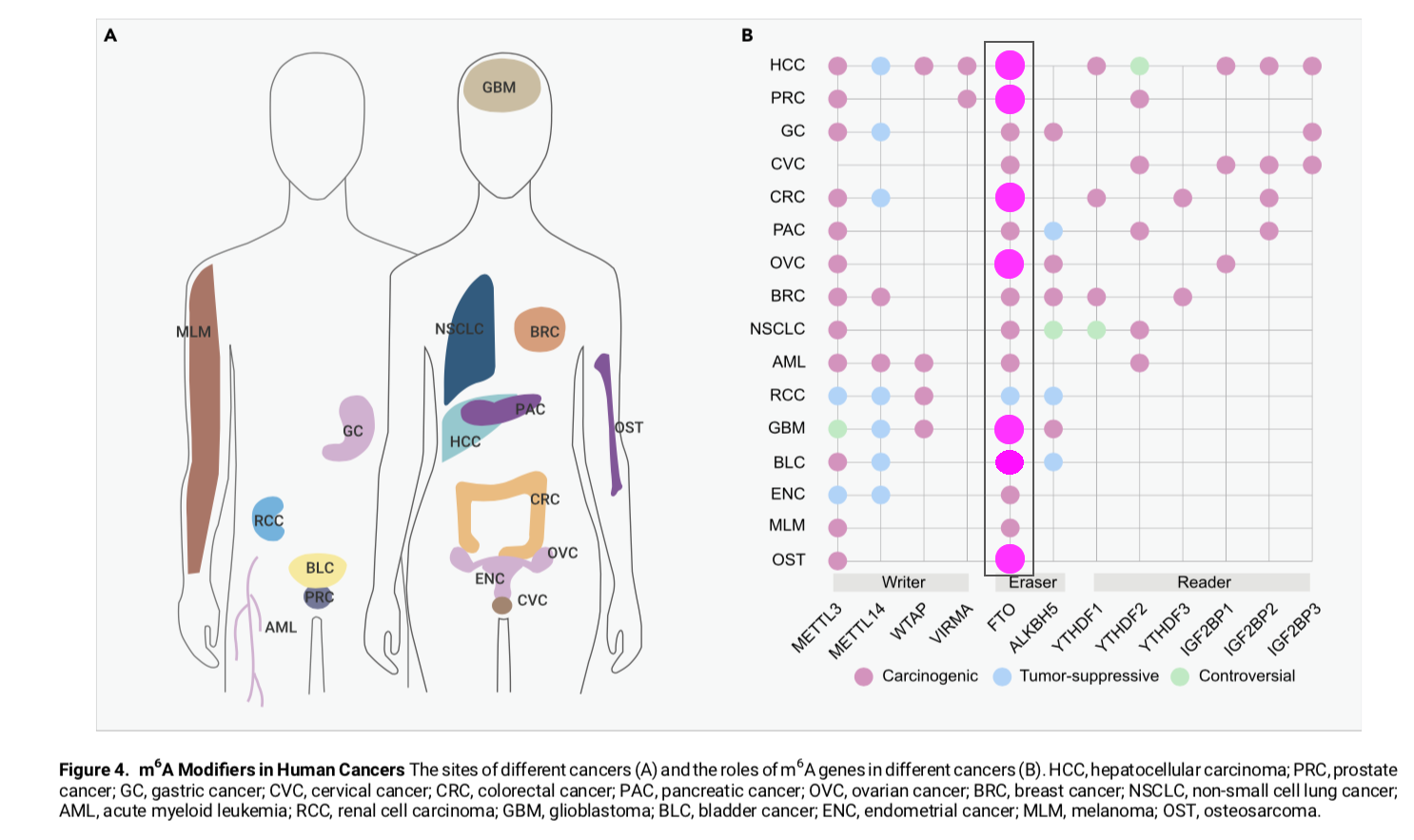
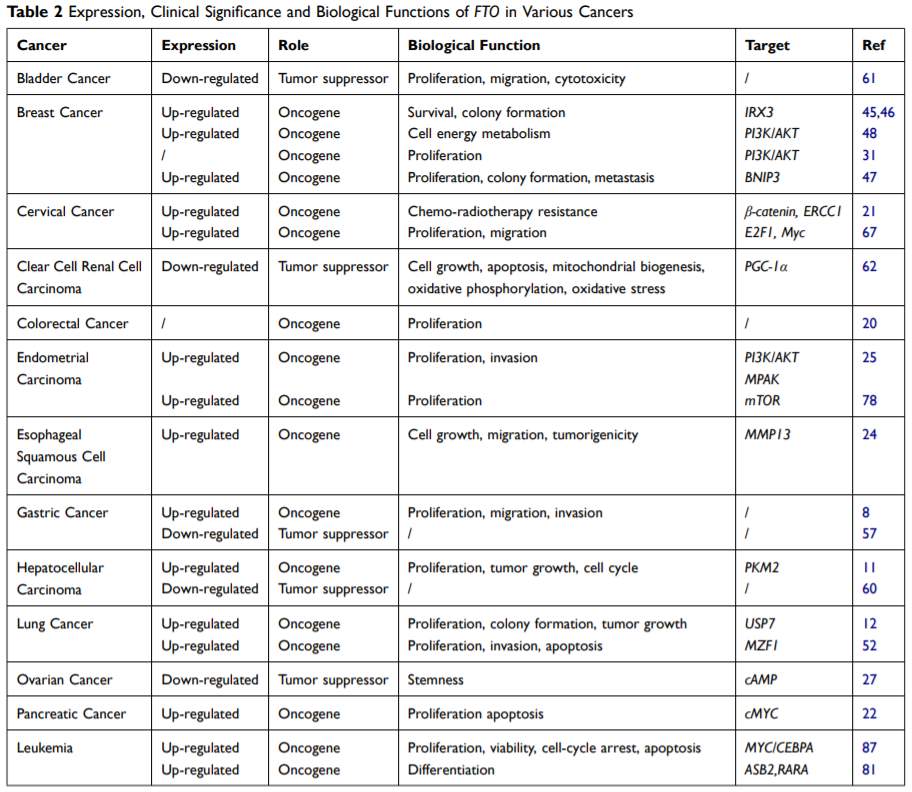
Originally, FTO was associated with obesity and type 2 diabetes, but after some research in 2009 linked the FTO A allele to the risk of some cancers, there was a spark of interest. Following on from 2009, the FTO protein has been linked to almost every cancer (Figure 1). Until recently, it was thought that FTO expression was not linked with bladder cancer, but that was proved otherwise in February of 2021 (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7851431/).
In 2020, there were an estimated 19.3 million new cancer cases. The most common cancers were female breast cancer (11.7% of cases), followed by lung (11.4%), colorectal (10.0 %), prostate (7.3%), and stomach (5.6%) cancers. All of which appear on the figure illustrated below. (https://pubmed.ncbi.nlm.nih.gov/33538338/). Total new cancer cases per year is expected to increase dramatically to 28.4 million by 2040.
Figure 1: List of cancers linked with FTO protein (recent bladder cancer reference not included in the 2nd image)
2.3 Cancer Drug Synergy
2.3.1 PD-1, PD-L1, and PD-L2 inhibitors
If you’re already out of your chair reading this, then that’s a good thing. If you have been paying attention, well, that’s even better. If you have, you will remember me talking about PD-1 inhibitors in the COH paper a couple pages up. Here, we are going to explore these in a little more depth and uncover why they are important.
PD-1 promotes an effective immune response against cancer, via the PD-1/PD-L1 pathway which controls the induction and maintenance of immune tolerance within the tumour microenvironment. The activity of PD-1 and PD-L1 control T cell activation, proliferation, and cytotoxic secretion in cancer to degenerating anti-tumor immune responses.
Rehashing what we have heard above, bisantrenes effect on FTO led to a significant reduction in the expression of PD-L1 and PD-L2. This effect has been replicated in two very recent studies:
(https://www.nature.com/articles/s41467-019-10669-0)
(https://www.sciencedirect.com/science/article/abs/pii/S0006291X20313711)
So, what these articles are suggesting is that the concentration (amount) of bisantrene in the cell at any one time can influence the concentration of PD-1 or PD-L1. And, more specifically, that inhibition of FTO will lead to inhibition of PD-1 and PD-L1. Now, if we take all of this information together, we can see that there is a dualistic effect if Bisantrene (an FTO inhibitor and thus also an inhibitor of PD-1 and PD-L1) is used in combination with a PD-1 inhibitor like Keytruda. There are multiple action points: 1) bisantrene inhibits FTO leading to inhibition of PD-1 and PD-L1, disrupting the PD-1/PD-L1 pathway; 2) bisantrene inhibits FTO protein leading to reduced HMA-induced drug resistance and potentially better efficacy of keytruda; 3) keytruda inhibits PD-1 directly, disrupting the PD-1/PD-L1 pathway. Please, keep in mind that this is speculative, or at least it will be for a short while until the results of the preclinical studies are released.
So, what’s the significance?
The 2019 sales and estimations on peak sales in 2026 for the two leading PD-1/PD-L1 inhibitors, Opdivo and Keytruda, are as follows:
2019
2026
Opdivo
USD 8.0B
~USD 11.75B
Keytruda
USD 11.1B
~USD 24.3B
If the relationship between bisantrene and a PD-1/PD-L1 inhibitor is found to increase the efficacy of PD-1/PD-L1 inhibitors, then the potential for sales increase is massive. Think of it as adding more fuel to the fire, with bisantrene being the fuel. What is important to note is that FTO has been linked to multiple cancers, many (all?) of which keytruda is FDA approved for. If found successful, the use of bisantrene and keytruda significantly improves the efficacy and ultimately the value of the drug and therefore is reflected in inherent value of the company, RAC.
2.3.2 TKI inhibitors
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6218444/pdf/41422_2018_Article_97.pdf)
Tyrosine kinase inhibitors (TKIs) inhibit tyrosine kinases, which are enzymes responsible for the activation of many proteins. Tyrosine kinases are genetically altered in cancer cells, as to impart a selection advantage for their cells survival and avoid death. While there have been many tyrosine kinase inhibitors (TKIs) that have entered the clinic, rapidly acquired resistance to TKIs represents a major hurdle for successful leukemia treatment.
The following abstracts are from papers that have found a relationship between FTO and TKI:
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6218444/pdf/41422_2018_Article_97.pdf)
(https://mcr.aacrjournals.org/content/early/2021/02/09/1541-7786.MCR-20-0541)
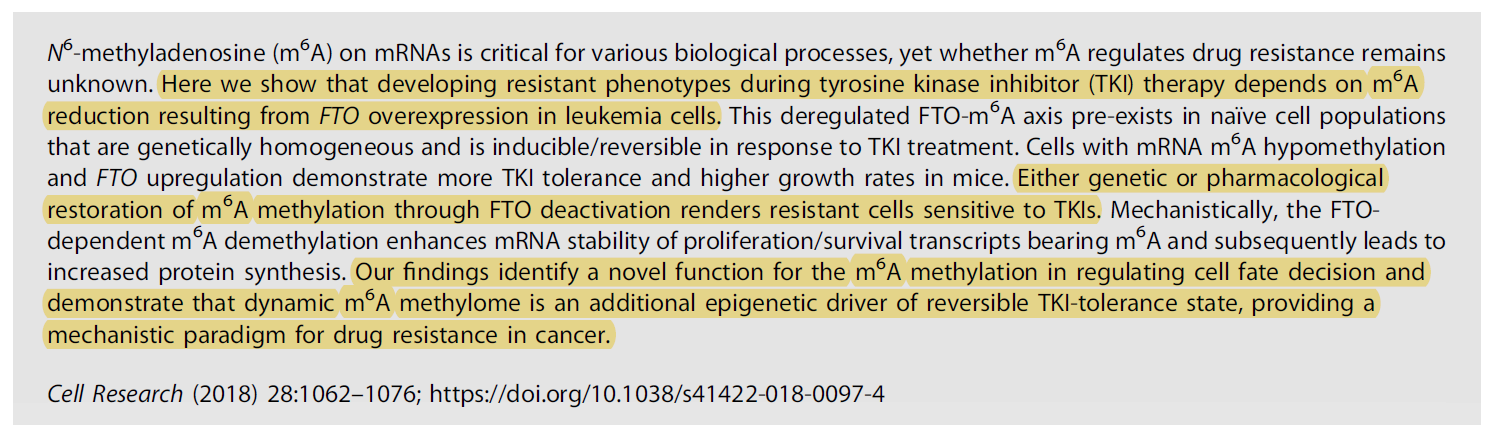
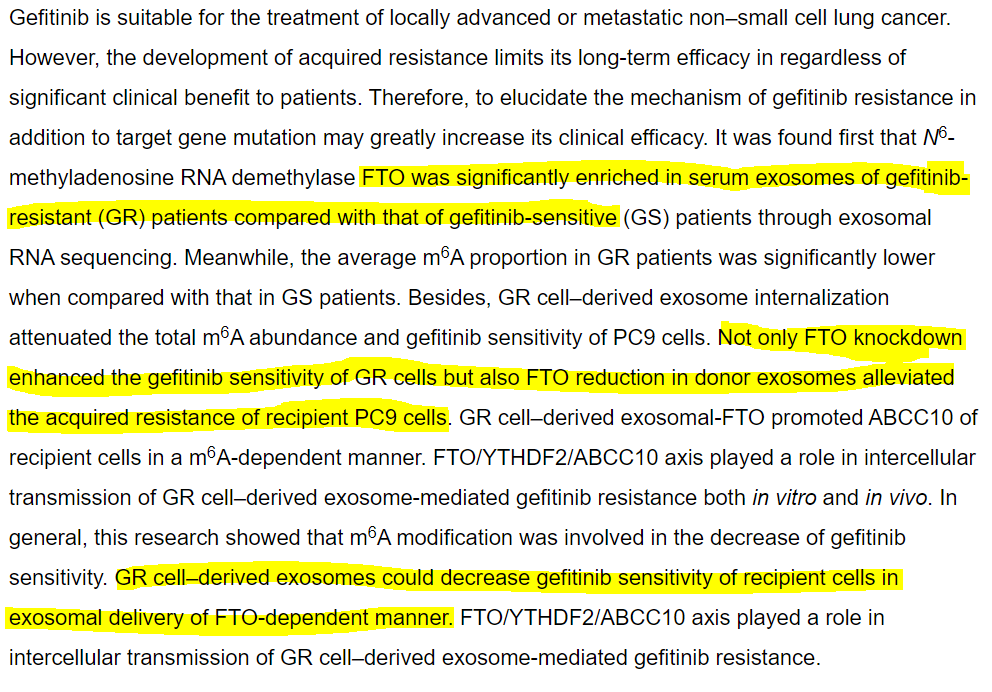
What these two papers are demonstrating is that FTO overexpression in cancerous cells leads to TKI resistance. The first paper is talking specifically about TKIs, while the second paper is talking about a specific drug (Gefitinib), which is an EGFR tyrosine kinase inhibitor - it’s a specific type of TKI. Both articles make the conclusion that inhibiting FTO increases the sensitivity to TKIs for cancerous cells.
2.4 FTO Inhibitor Comparison
Due to the substantial amount of information that has come out as of late, there has been a surge of research trying to elucidate a potent FTO inhibitor (COH paper included). The purpose of this section is to compare what is known about bisantrene at this very point in time and compare it to other ‘FTO inhibitors’ out there. I present the word FTO inhibitors in inverted commas because I believe bisantrene is in a class of its own, anyway...
2.4.1 CS2 or Brequinar
This is for everyone scratching their heads about CS2 or Brequinar, the other drug mentioned in the COH paper.
The main issue with cancer drugs is getting the results in the clinic with human patients. This is where CS2 or Brequinar failed and why it is not an alternative for FTO inhibition. It failed as an anticancer agent, when it was used in more than 250 patients and it also failed as an transplant organ rejection drug (it is very immunosuppressive). One of the primary reasons Brequinar did not make it to market as an anti-rejection drug was that plasma concentration os brequinar would vary enormously (~10 fold) depending on the patient. This meant that doses had to be adjusted for each patient based on their blood work, which made brequinar impractical to use in regular clinical practice and is likely the reason why it was dropped.
2.4.2 FTO-04
This paper was released on the 7th of January 2021. In short they are trying to develop a novel FTO inhibitor. However, I am dubious of their transparency, as bisantrene or the COH paper are not mentioned anywhere and they state that current FTO inhibitors are unsuitable for clinical applications. I need not go far for a simple explanation and that is because the CoH paper came out as this study was being completed and, in my opinion, completely undermines their findings – let’s take a look shall we. There are two key comments highlighted in the abstract below that I would like to address and unpack for you that gives some insight into the comparison between the FTO-04 and bisantrene.
(https://pubs.acs.org/doi/pdf/10.1021/acschembio.0c00841)
“However, current FTO inhibitors are unsuitable for clinical applications due to either poor target selectivity or poor pharmacokinetics.”
Firstly, we’ll discuss what each of these points mean: 1) target selectivity is referring to the sensitivity of FTO inhibitors to bind to the FTO protein; and 2) pharmacokinetics refer to the drug utilization in the body which can be better described by the overall safety and efficacy of the drug when ingested into the body.
Target selectivity:
This research clearly has not looked at the COH paper, probably because it undermines their entire study and months of hard work. The researchers from COH state clearly “These data suggest that CS1 and CS2 selectively bind to and occupy the catalytic pocket of FTO and thereby block m6A-modified oligos from entering into FTO’s catalytic pocket”. Additionally, the paper listed above states that their drug FTO-04 reported significant selectivity over ALKBH5 (another known M6A demethylase), however, the CoH paper states that Bisantrene did not suppress enzymatic activity and further states that Bisantrene has selectivity against FTO specifically. Based on the commentary between these two articles, it seems as though Bisantrene is more selective against FTO.
Pharmacokinetics:
If you have read the introduction, you will be more than aware of not only the efficacy of bisantrene but also the safety data that has been collected in over 2000 patients. Indicating that bisantrene pharmacokinetic profile is far more advanced than all of the FTO inhibitors researched in this paper. However, as a caveat, I will notably agree that bisantrene is yet to provide pharmacokinetic properties relating directly to its use as an FTO inhibitor.
“Rational design of 20 small molecules with low micromolar IC50’s and specificity toward FTO over ALKBH5 identified two competitive inhibitors FTO-02 and FTO-04.”
I would like to address the IC50 values mentioned in this second highlighted section. The Huff et al. paper states their FTO-04 has comparable IC50 values to the FB23-2 inhibitor (an inhibitor studied in a ~2018 paper), which is 10 to 30- fold higher than values used for bisantrene. Bisantrene was an effective FTO inhibitor with IC50 values in the nanomolar ranges (FTO-04 was in the microMolar ranges). Now, for the math aficionados who are interested – 1 microMolar (uM) is 1000 nanoMolar (nM). This highlights the substantial IC50 values of Bisantrene and is a significant positive for our drug and aspirations of the future.
In conclusion, bisantrene is a drug that selectively binds better, is pharmacokinetically more suited, and requires 10 to 30-fold lower concentrations to inhibit FTO than FTO-04. Additionally, preclinical concepts like FTO-04 take years to go from development through to safety and efficacy in trials, whereas bisantrene has already been through rigorous phase I and phase II trials demonstrating safety and efficacy. Bisantrene isn’t one step ahead of the game, it’s 50.
2.4.3 FB23-2
(https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6812656/pdf/nihms-1053837.pdf)
The FB23-2 molecule is a derivative of the meclofenamic acid (MA), which selectively inhibits FTO. The major comparisons that I would like to make about this molecule is the IC50 values required for efficacy and the pharmacokinetics.
IC50 values
This study suggests that the IC50 values required to inhibit the proliferation (multiplication of cells) ranged from 1.9 uM to 5.2 uM (or 1900 nM to 5200 nM). In comparison, bisantrene required IC50 values ranging from 22.0 nM to 175.9 nM (or 0.022 uM to 0.175 uM) to half maximal inhibit cell viability (Figure 1). To put this into perspective for you 1uM of FB23-2 is equal to 1000nM of bisantrene. Now, I understand that proliferation (multiplication) and cell viability (number of living cells) are completely different things, but what it does show is the difference in IC50 value required for a significant effect.
Figure 1: Comparison of FB23-2 (left) and bisantrene (CS1; right) half maximal inhibitory dose.
Pharmacokinetics
As mentioned above, bisantrene has been safely and efficaciously used in multiple phase I and II trials and is 50 steps ahead of the game in comparison to a preclinical concept like this.
2.5 FTO Conclusion
In conclusion, from 260,000 other compounds bisantrene was found to be the best FTO inhibitor. It also has the potential to make other important and highly valuable drugs work better and is pharmacokinetically and clinically more viable than other preclinical FTO inhibitors in the research world today. The year of 2021 will be monumental for the future of bisantrene and shareholders of RAC.















Add to My Watchlist
What is My Watchlist?
 (20min delay) (20min delay)
|
|||||
|
Last
$2.57 |
Change
-0.010(0.39%) |
Mkt cap ! $446.6M | |||
| Open | High | Low | Value | Volume |
| $2.68 | $2.68 | $2.37 | $2.089M | 834.4K |
Buyers (Bids)
| No. | Vol. | Price($) |
|---|---|---|
| 1 | 1943 | $2.57 |
Sellers (Offers)
| Price($) | Vol. | No. |
|---|---|---|
| $2.59 | 15000 | 2 |
View Market Depth
| Last trade - 16.10pm 18/09/2025 (20 minute delay) ? |
| RAC (ASX) Chart |