I’d recommend sitting down and putting your reading glasses on for this one.
In preparing for the CPACS trial, I have uncovered research with significant implications for Bisantrene's clinical and commercial future. My evaluation process for the commercial potential of biotechnology companies includes: 1) assessing the total addressable market, 2) identifying clinical and/or commercial competitors, 3) comparing the test drug to these competitors, and 4) determining if the clinical efficacy is sufficient to drive commercial outcomes. This methodology helps evaluate the risk versus reward, vital for success as the most successful oncology drugs capture large markets first and sustain standard of care status.
Recently, the m6A mRNA pathway has attracted considerable interest, with numerous groups developing FTO inhibitors, presenting a clinical and commercial risk to RAC. Thus, continuous evaluation is crucial to ensure a seamless path to success. While there are few FTO inhibitors sensitive enough at the nM concentration to be a serious threat, new findings suggest additional clinical challenges with FTO inhibition could arise.
FTO protein plays a role in gene transcription and cellular function by demethylating m6A. FTO inhibitors, by blocking this demethylation, can alter gene transcription significantly. Given that many aggressive and resistant cancer forms (over 28 types) exhibit high FTO expression and depend heavily on hyper-demethylation, they are particularly vulnerable to FTO inhibitors. This sensitivity makes FTO a promising therapeutic target, especially as cancer stem cells, often responsible for cancer relapse, typically show high FTO expression. The clinical history of Bisantrene suggests it is on track to becoming a first-in-class and best-in-class drug for the potent inhibition of the FTO protein.
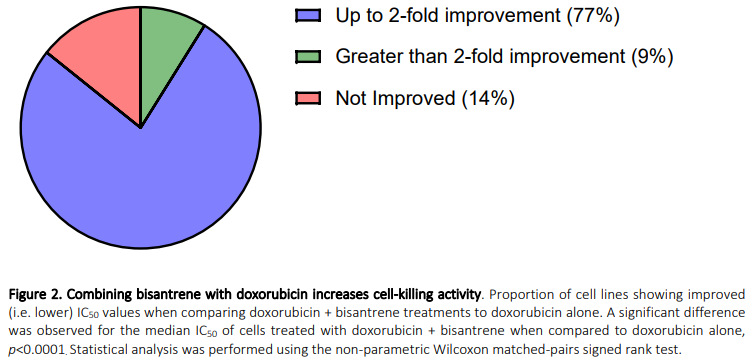
Cardiotoxicity remains a significant challenge in oncology, with decades of management but few robust solutions. Anthracyclines like doxorubicin are highly effective but notoriously cardiotoxic. Research indicates that cancer cells resistant to anthracyclines can be re-sensitized through FTO inhibition, which re-establishes their vulnerability to these drugs. In a metaphorical sense, think of FTO as a stone wall that cancer cells erect against doxorubicin, and Bisantrene as the Grond (IYKYK) that breaches this barrier, allowing the anthracycline to be effective once again. Preclinical studies by RAC show that Bisantrene enhances doxorubicin's efficacy in 86% of the 143 tested cancer cell lines.
While FTO inhibition is demonstrating excellent preclinical potential in treating cancer, there is an accumulating body of research that has investigated the role of FTO in cardiotoxicity. The following lines of evidence are extremely important for investors to familiarize themselves with. It is difficult for me to explain my excitement with these discoveries, as it has the potential of isolating Bisantrene as a cardioprotective FTO inhibitor. I have done the best I can to keep the following information simple and I have taken much time to capture and highlight elements that explain these concepts. Briefly, FTO knockdown is shown to synergise with cardiotoxic agents to further kill heart cardiomyocytes (HCM).
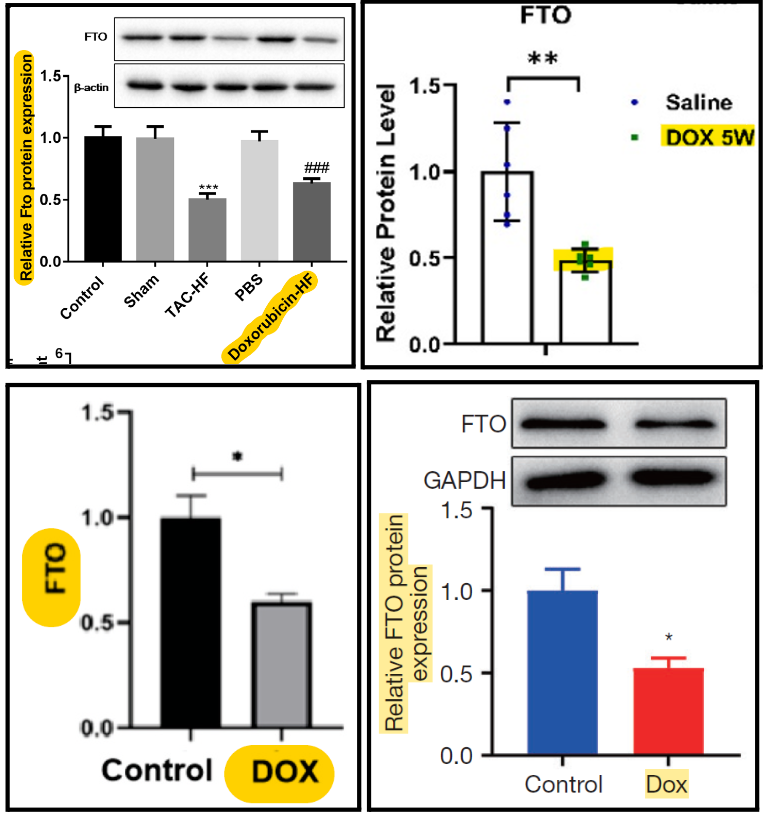
FTO expression levels decrease in HCM treated with DOX
The expression level of FTO was decreased across all four studies investigating m6A proteins in DOX treated HCM. FTO protein levels are decreased in DOX-treated cardiomyocytes primarily due to the drug’s impact on the cellular mechanisms that control gene expression through m6A methylation.
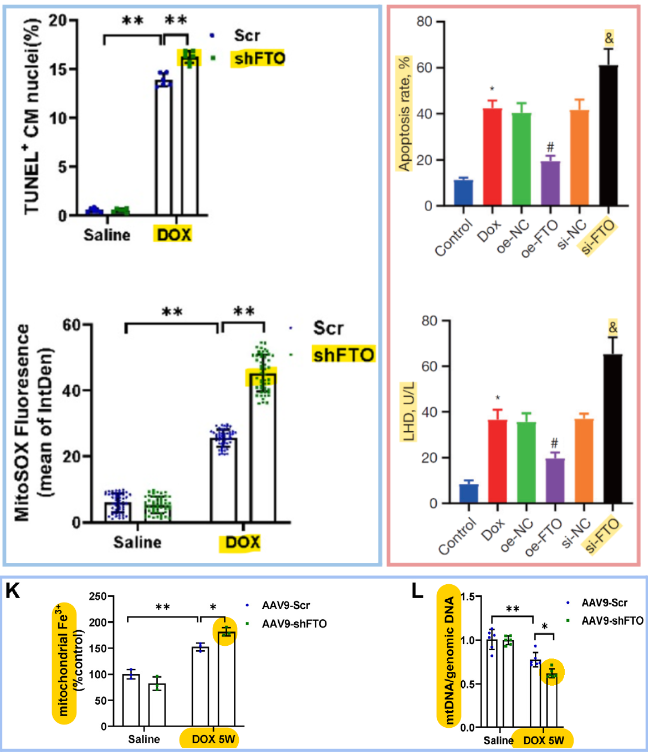
Further FTO knockdown increase HCM cytotoxicity of DOX
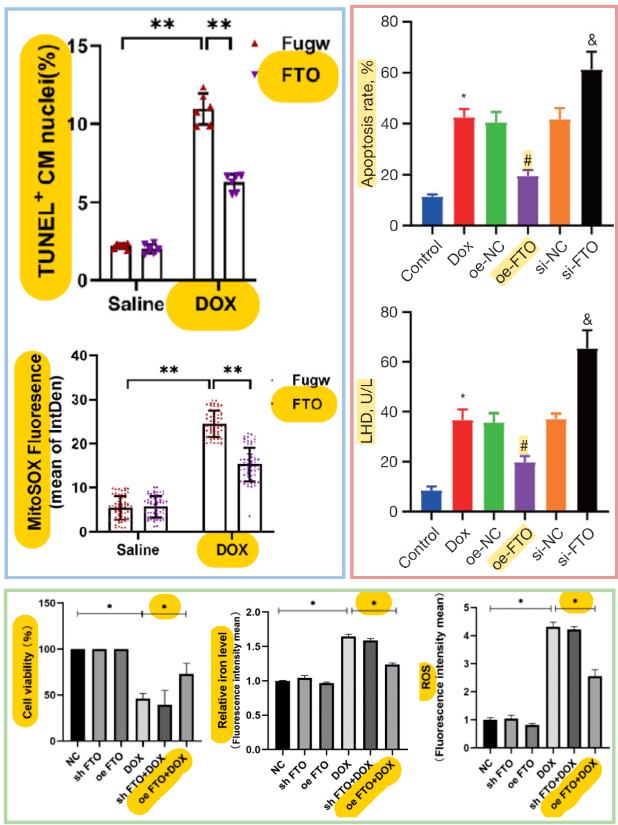
FTO knockdown increases HCM apoptosis (cell death), oxidative stress, and mitochondrial stress (blue border) and increases apoptosis, LDH (a marker of cell death and/or tissue damage), and inflammatory markers (red border; other inflammatory markers not shown).
While FTO knockdown has been shown to synergise with DOX cardiotoxicity in vitro, FTO knockdown on its own demonstrated no signs of cardiotoxicity.
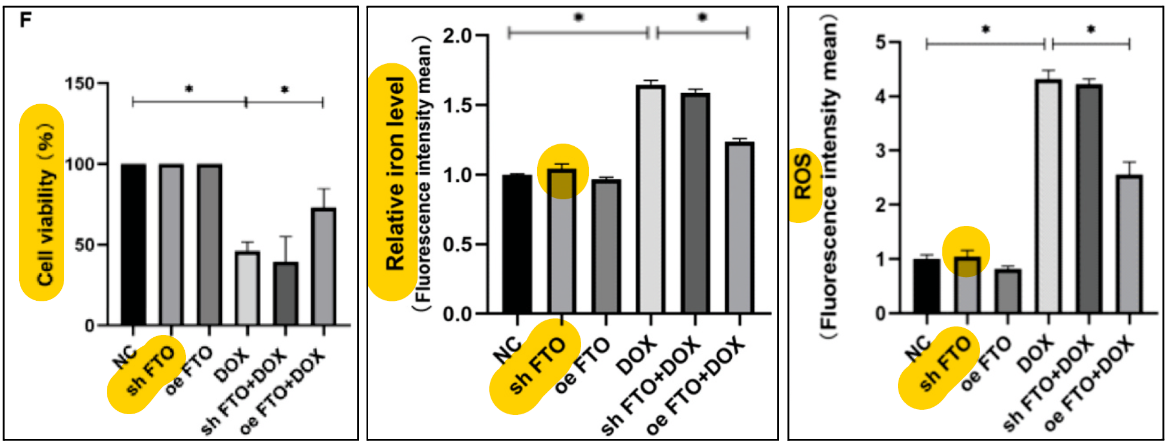
FTO overexpression rescues HCM cytotoxicity of DOX
FTO overexpression decreases HCM apoptosis (cell death) and oxidative stress (blue border), decreases apoptosis, LDH, and inflammatory markers (red border; other inflammatory markers not shown), and increases cell viability while decreasing Fe2+ and ROS production (green border).
https://pubmed.ncbi.nlm.nih.gov/33548009/
https://www.sciencedirect.com/science/article/pii/S2452302X22004636
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10904293/pdf/cdt-14-01-158.pdf
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10862061/pdf/main.pdf
FTO inhibitors decrease cell viability in DOX treated HCM
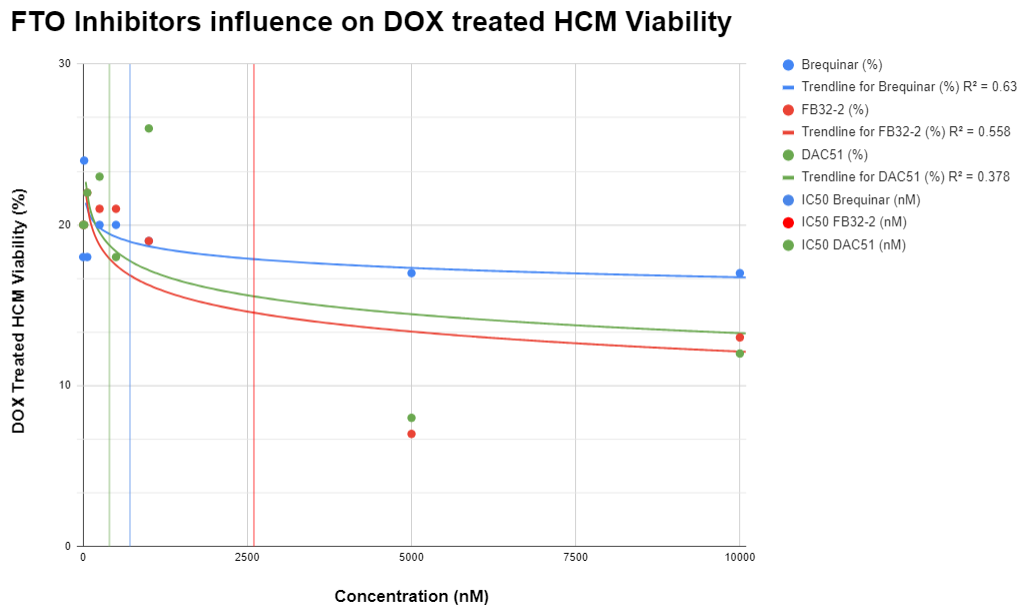
RAC published research indicating none of the competitor FTO inhibitors provide cardioprotection in DOX-treated HCM. Below is a graph that evaluates the three FTO inhibitors Brequinar, FB32-2, and DAC51 on DOX treated HCM viability. Data points are taken directly from the RAC announcements where values are the average of three full replicates, each performed in triplicate. All three FTO inhibitors have a negative correlation with dose and cell viability, whereby as the dose of FTO inhibitor increases, DOX treated HCM viability decreases. After the specific IC50 values are met, all FTO inhibitors display a general downwards trend away from the starting ~20% cell viability, indicating synergy with DOX and further cardiotoxicity.
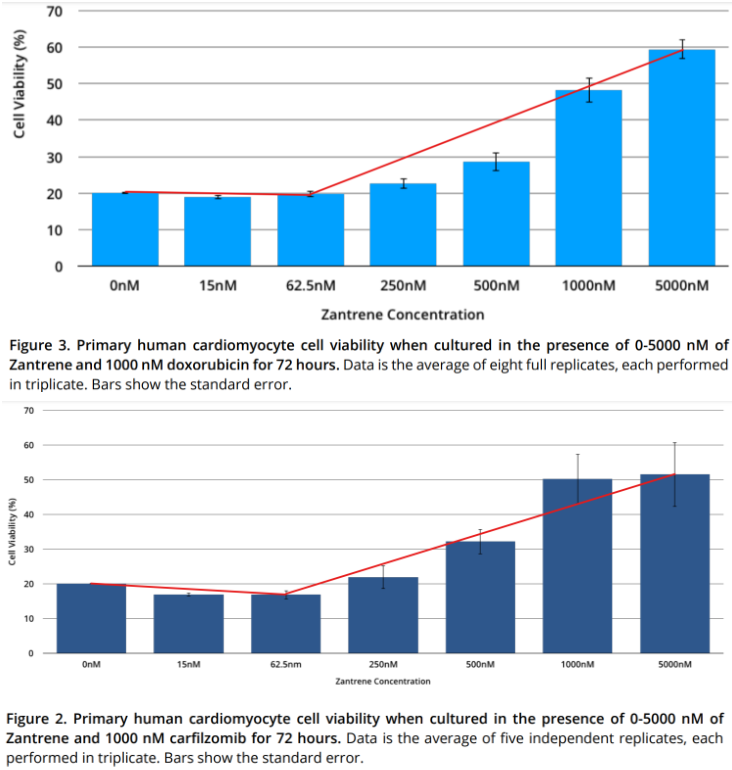
Bisantrene improves cell viability in DOX and Carfilzomib treated HCM
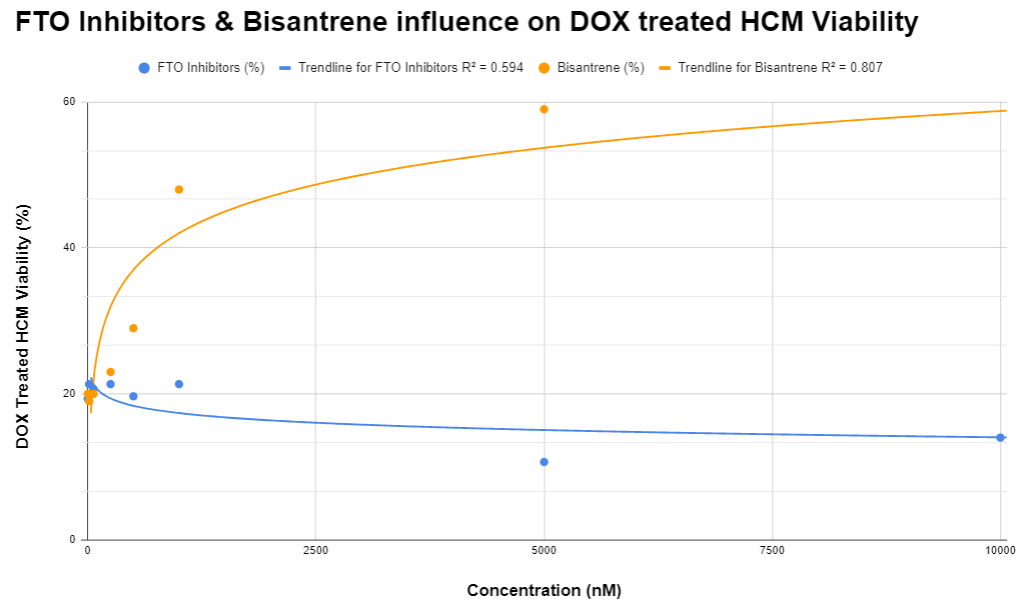
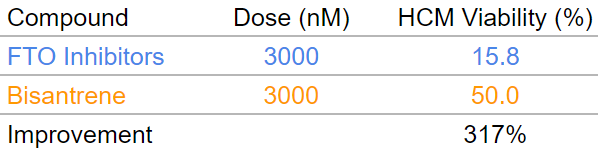
While the 3 tested FTO inhibitors demonstrate a tendency towards additional cardiotoxicity, Bisantrene trends in the opposite direction and has a positive correlation between dose and HCM viability. Below is a graph that compares the average of the three FTO inhibitors to Bisantrene (averages of eight full replicates, each performed in triplicate) on DOX treated HCM viability. Visually, the log trendlines oppose each other, with Bisantrene demonstrating clear improvements in DOX treated HCM viability. This highlights that cardioprotection and FTO inhibition of Bisantrene is mutually exclusive, and that the cardioprotective MoA(‘s?) is of measurable significance to overcome the additional toxicity associated with combination DOX and the FTO inhibitor element of Bisantrene. At a dose of 3,000nM (~200 mg/m2), Bisantrene provides a 317% improvement in cell viability than the averages of three competitor FTO inhibitors in DOX-treated HCM (table below generated from the logarithmic equations based on averages for Bisantrene and FTO inhibitors).
Table: Comparison of DOX treated HCM viability at 3,000nM dose for Bisantrene & FTO inhibitors
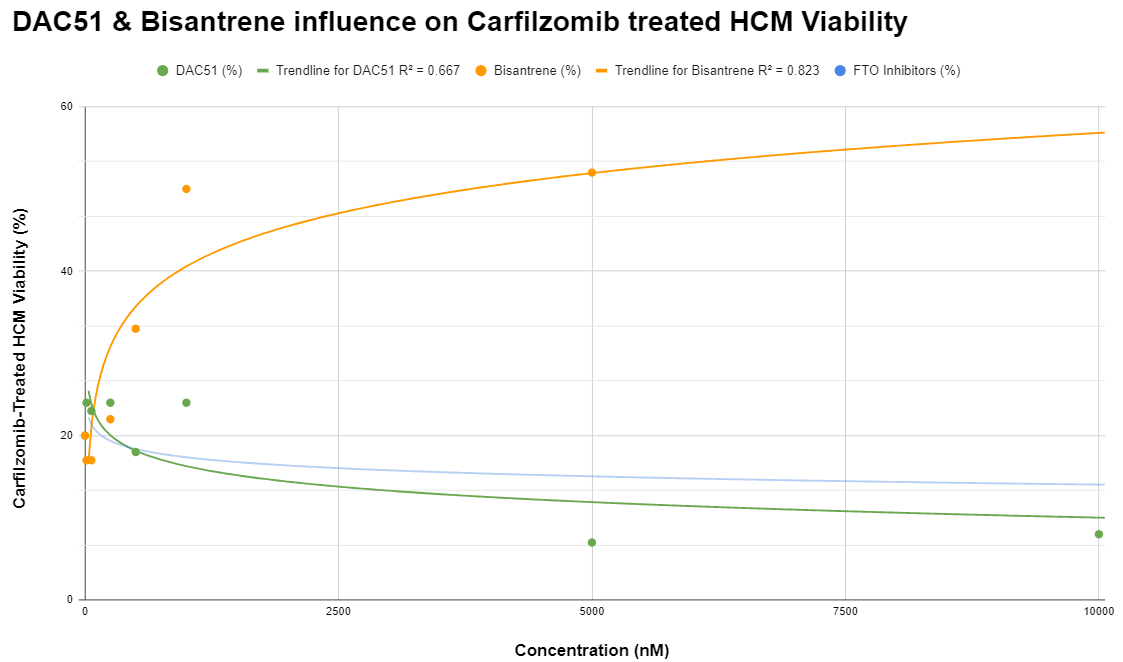
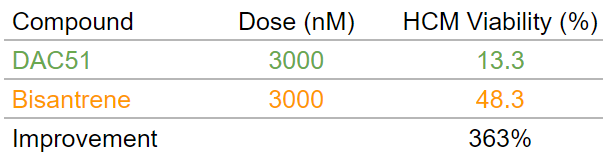
A similar trend was observed in carfilzomib-treated HCM between the FTO inhibitor DAC51 and Bisantrene. DAC51 decreased cell viability in carfilzomib-treated HCM, with a trend similar to DOX-treated HCM (light blue line). Bisantrene increased cell viability in carfilzomib-treated HCM, similar to the trend observed in DOX-treated HCM. At a dose of 3,000 nM (200 mg/m2), Bisantrene provides a 363% improvement in cell viability than DAC51 in carfilzomib-treated HCM (table below generated from the logarithmic equations based on averages for Bisantrene and DAC51). Once again, this highlights mutual exclusivity of the cardioprotective MoA(‘s?) and FTO inhibition, and the cardioprotective MoA(‘s?) is of measurable significance to overcome the additional cardiotoxicity associated with combination carfilzomib and FTO inhibition.
Table: Comparison of Carfilzomib treated HCM viability at 3,000nM dose for Bisantrene & DAC51
The parallel reactions observed in HCM subjected to DOX and carfilzomib treatments when treated with FTO inhibitors and Bisantrene underscore the potential clinical drawbacks of utilizing FTO inhibitors, while simultaneously indicating a distinct therapeutic niche for Bisantrene.
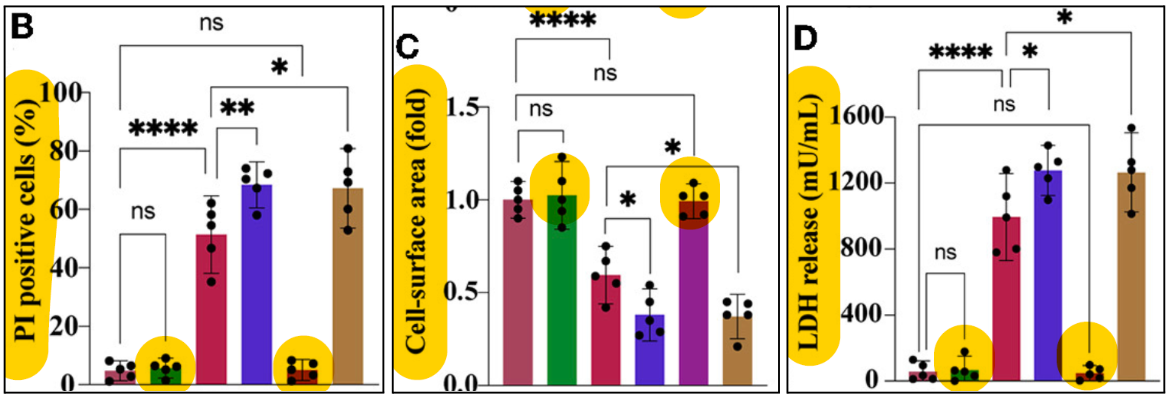
FTO mediates tyrosine-kinase inhibitor (TKI) cardiotoxicity
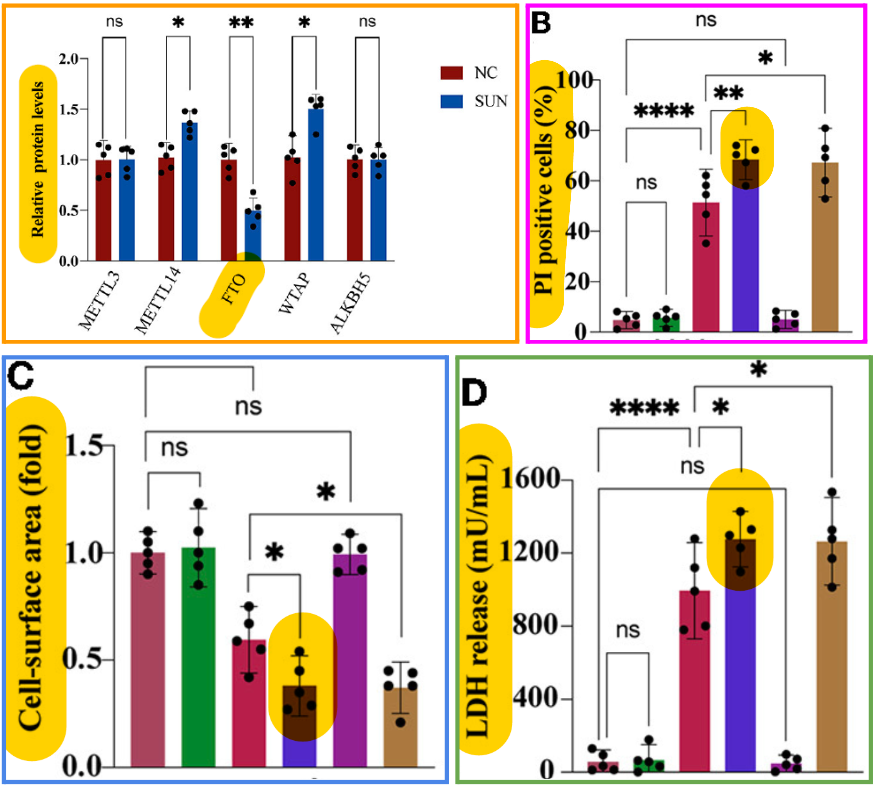
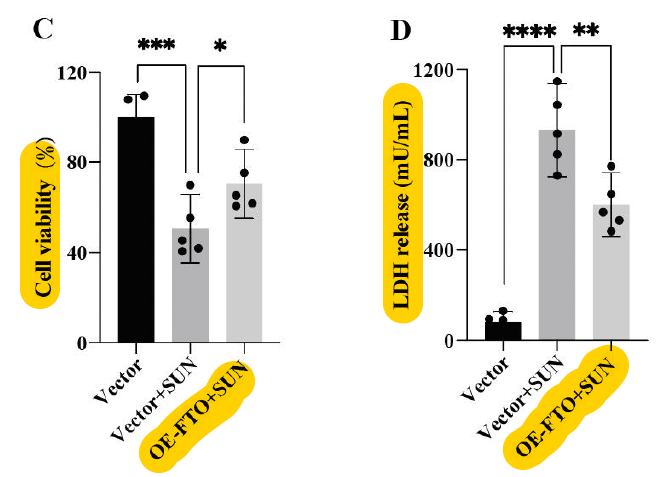
Recent research has found that FTO is an influential target for TKI therapy in HCM cardiotoxicity. Similar to DOX- and carfilzomib-treated HCM, FTO was found to be downregulated in TKI-treated HCM (orange border). Additionally, the FTO inhibitor FB32-2 or FTO knockdown models synergised with the TKI inhibitor Sunitinib to kill more HCM (pink), decreased cell surface area (blue), and increased LDH (green border). Forced overexpression of FTO rescued cell viability and decreased LDH release in Sunitinib treated cells (red border). This data together indicates that FTO inhibition aggravates TKI cardiotoxicity. This research highlights the synergistic nature of FTO inhibitors when used in conjunction with cardiotoxic agents. The funny thing about this research is that if they had used Bisantrene, they would have seen opposite effects.
While FTO knockdown/inhibition has been shown to synergise with TKI inhibitors for cardiotoxicity in vitro, FTO knockdown/inhibition on its own demonstrated no signs of cardiotoxicity.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8985653/pdf/fcvm-09-849175.pdf
A summary of data so far
While targeting the m6A mRNA pathway with FTO inhibitors is proving to be an effective and exciting therapy option with a lot of clinical and commercial potential, it appears the increased risk of cardiotoxicity may limit their use in the clinic, particularly in combination with cardiotoxic drugs. If FTO inhibition synergises with cardiotoxic drugs to increase rates of cardiotoxicity, I believe it will limit their use in the clinic, decreasing the clinical and commercial competitors for Bisantrene and RAC. At the very least, these discoveries of synergism with cardiotoxic drugs in HCM increase the clinical risk for FTO inhibitors to be successful in combination.
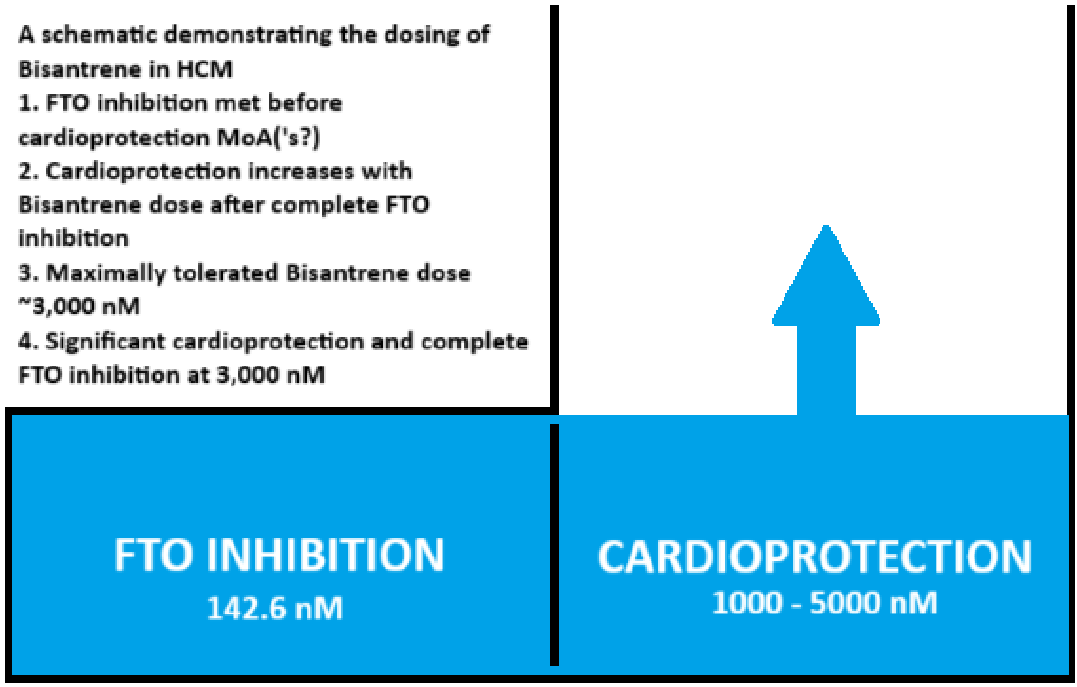
Bisantrene dosing for FTO inhibition and cardioprotection
I have used a J-shaped mug analogy to oversimplify the nuanced interplay between the two therapeutic targets of Bisantrene, providing an accessible visual for understanding how incremental increases in drug dosage can lead to progressive clinical outcomes, from FTO inhibition to cardioprotection.
Bisantrene exhibits a dual mechanism of action that is dose-dependent. At lower concentrations, specifically around 142.6 nM, Bisantrene rapidly achieves complete inhibition of the FTO protein. This early effect is akin to filling a small compartment in a J-shaped mug – it doesn't take much 'water' (or dosage) for this compartment to reach its capacity (below). Once the threshold for FTO inhibition is met, any additional Bisantrene begins to overflow into a larger, adjoining compartment that represents cardioprotection. This second compartment requires a larger volume to fill, indicative of the higher doses of Bisantrene needed to confer cardioprotective benefits. These cardioprotective effects become evident within a dosage range of 1000 to 5000 nM. The maximally tolerated dose for Bisantrene in humans is roughly around 3000 nM, where there is significant protection of heart tissue along with sustained FTO inhibition. It’s important to note that the maximally tolerated dose reflects the highest dose that patients can safely receive without adverse effects, and it may differ from the optimal therapeutic dose, which must be fine-tuned to balance efficacy and patient safety.
Bisantrene is in a great position clinically, as the IC50 for FTO is lower than the expected IC50 for cardioprotection. This means that synergy for cancer killing can be achieved early in the dosing regimen (oncology drugs drive the largest commercial outcomes), and dose can continue to be increased providing more and more cardioprotection until the maximal tolerated dose.
The RAC generated DOX & Carfilzomib data demonstrate this phenomena, whereby measurable cardioprotection occurs from 500 nM of Bisantrene in HCM. Once again, the cardioprotection MoA(‘s?) must be of significance to overcome the synergy cardiotoxicity of FTO inhibitors and DOX or Carfilzomib.
Clinical data evaluating the cardiotoxicity of FTO inhibitors
I conducted a review of clinical data for the known FTO inhibitors, which was limited to Brequinar and Bisantrene.
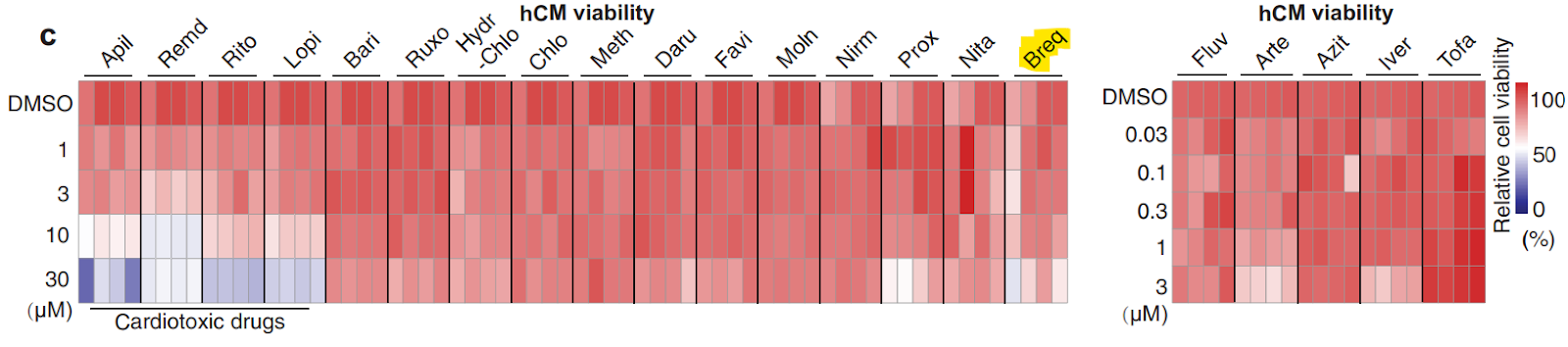
While there is no clinical evidence for cardiotoxicity, brequinar was investigated in a panel of covid drugs evaluating their cardiotoxicity. The heat map below is a visual way of representing cardiotoxicity, with red indicating no cardiotoxicity and blue cardiotoxic. Brequinar is highlighted and is not cardiotoxic, which is what you would expect from a single agent semi-potent FTO inhibitor.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9539280/pdf/ADVS-9-2203388.pdf
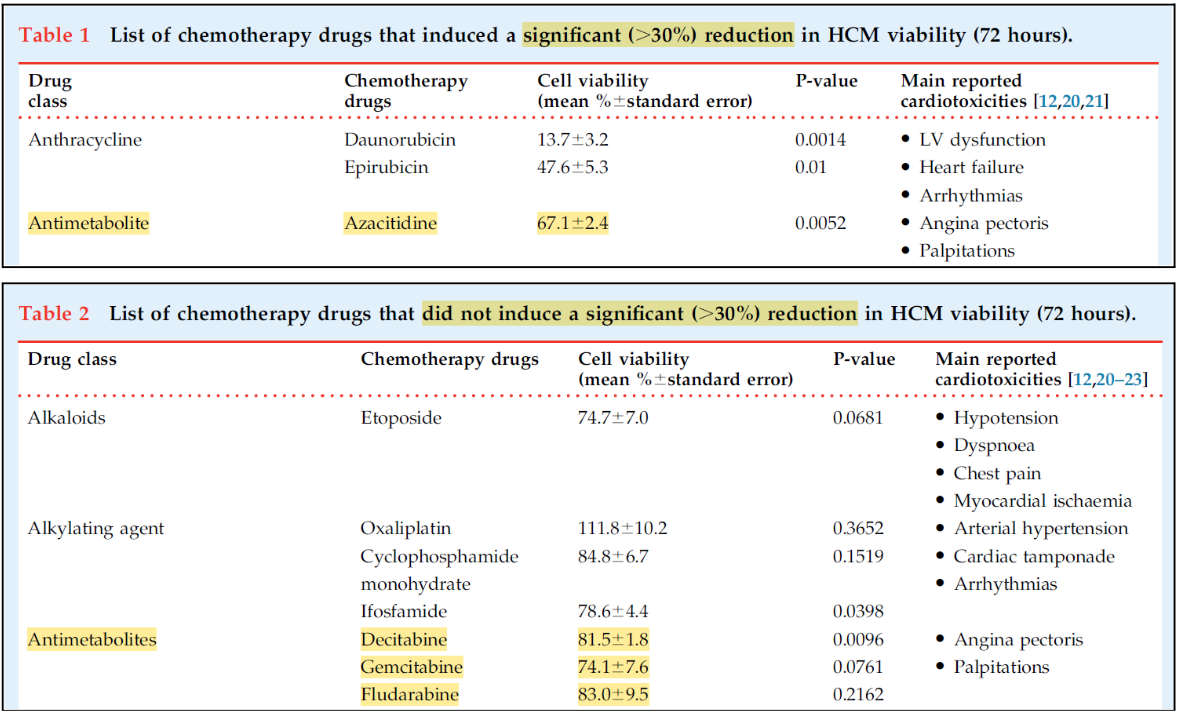
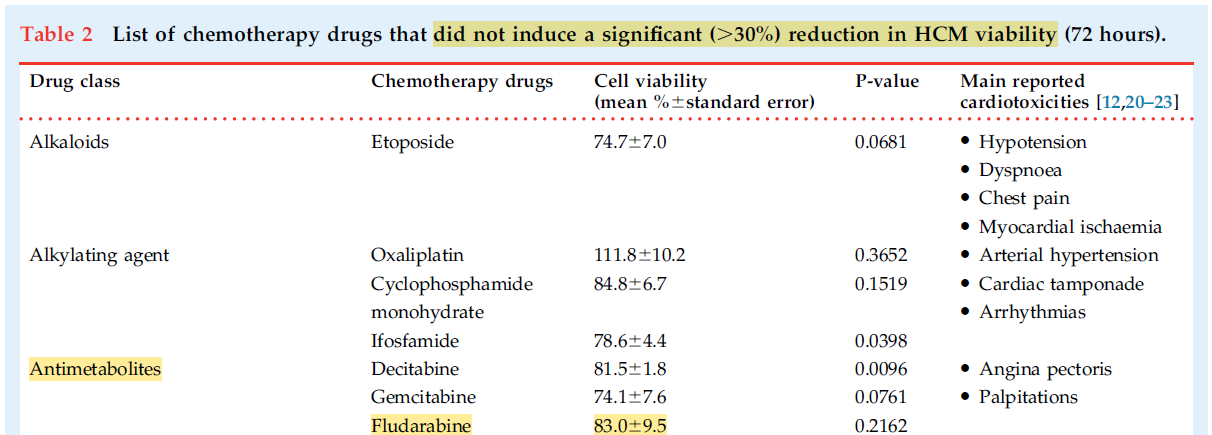
For Bisantrene, the phase II trial in a heavily pretreated, relapsed/refractory pediatric population with Aracytine (Ara-C) and the phase II trial in heavily pretreated, relapsed/refractory patients in combination with Fludarabine and Clofarabine are the only combination trials available to me. Ara-C, clofarabine, and fludarabine are antimetabolites, which is a drug class that has demonstrated variable cardiotoxicity. The Doan et al paper demonstrates Azacitidine produces a significant reduction in HCM viability, while decitabine, gemcitabine, and fludarabine provide more modest cardiotoxicity.
Bisantrene in Combination with Fludarabine and Clofarabine As Salvage Therapy for Adult Patients with Relapsed or Refractory Acute Myeloid Leukemia (AML)
Bisantrene in combination with clofarabine and fludarabine achieved a 40% response rate (CR=33.3%, PR=6.7%) in a heavily pretreated patient population. The median patient age was 48 years (range 19-69) and the median number of prior lines of therapy was four (range 3-9). All patients were refractory to prior regimens, which included cytarabine and daunorubicin; fludarabine, cytarabine, idarubicin, and granulocyte colony-stimulating factor (FLAG-Ida), venetoclax; azacitidine; gilteritinib, radiation therapy, and CAR-CD19 for 8:21 (genotype) AML.
While there is no information that I can find on the role FTO plays in response to the antimetabolites fludarabine or clofarabine in AML cells, there is data supporting FTO upregulation in response to the following treatments:
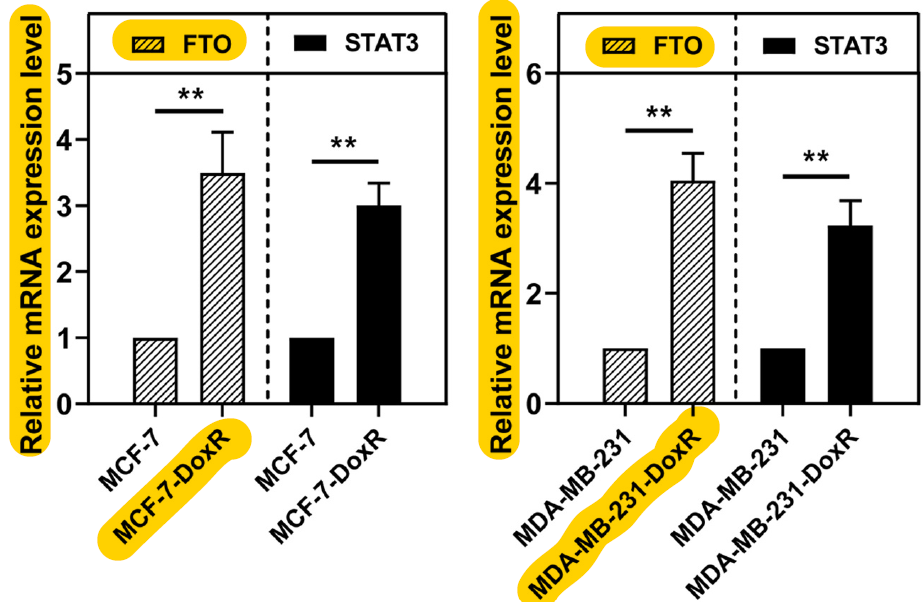
Anthracyclines (Daunorubicin & Idarubicin): FTO overexpressed in response to Doxorubicin.
Antimetabolites (Cytarabine (Ara-C), Fludarabine, & Azacitidine): FTO overexpressed in response to Ara-C.
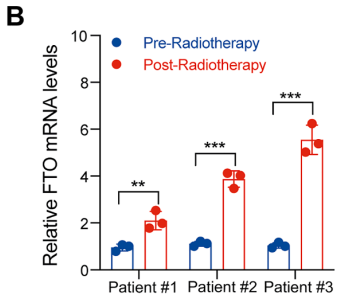
Radiation Therapy: FTO overexpressed in response to radiotherapy.
It is up to investors to determine whether or not patients who responded to treatment had cancers that were overexpressing FTO. My position is that Bisantrene, functioning as an FTO inhibitor, synergised with the antimetabolites fludarabine and clofarabine to overcome chemoresistance and kill cancers who were being driven by FTO. The rational for my decision includes Bisantrene being the most potent inhibitor of the FTO protein and an extremely poor anthracene, patients are refractory to anthracenes as well as a number of other treatments shown to upregulate FTO in response to treatment, an FTO inhibitor only now being used as a therapeutic agent, patients responding to treatments they were previously refractory to, FTO upregulation is a common response to prior chemotherapy used, and the dosing regimen sufficient to inhibit the FTO protein in patients. To achieve a 40% response rate in this heavily pretreated patient population is an incredible result for RAC and Bisantrene, but I do wonder what an improved screening process for patients (including only patients where FTO is driving tumorigenesis) as well as a dosing regimen that effectively inhibits the FTO protein for a sufficient time to prevent the hallmarks of cancer and overcome chemoresistance.
Fludarabine has been shown to be marginally cardiotoxic (below), decreasing HCM viability to 83% (+- 9.5%). I could not find meaningful data to support the cardiotoxicity of fludarabine in patients other than some case reports.
Clofarabine has established cardiotoxicity in patients causing cancer-therapy related cardiac dysfunction in >10% of cases, though it is impossible to know the true effects due to lack of adequate screening.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8352330
https://link.springer.com/article/10.1007/s12325-023-02696-7
The evidence so far suggests FTO knockdown models synergise with TKI inhibitors, anthracyclines, and proteasome inhibitors to produce greater levels of cardiotoxicity in HCM. It is up to investors to assume whether FTO inhibition conferred by Bisantrene synergised with the slight cardiotoxicity of fludarabine and established moderate cardiotoxicity of clofarabine in heart cardiomyocytes of heavily pretreated patients, and whether Bisantrene’s cardioprotection MoA(‘s?) played a role in preventing clinical signs of cardiotoxicity. The fact that there were no clinically relevant cardiotoxic events and no patient developed ECG changes is unequivocal - the biological reasoning is up to each investor to decide.
Based on many lines of evidence, it is my belief that Bisantrene in combination with clofarabine and fludarabine achieved a 40% response rate in heavily pretreated, relapsed and refractory patients with no clinically relevant cardiotoxicity due to FTO inhibition of cancer alongside cardioprotective mechanisms within heart cardiomyocytes.
A phase II study of Bisantrene in combination with high dose Ara-C in heavily pretreated pediatric population
Bisantrene in combination with high dose (HD) Ara-C recorded a 46% complete response rate and no cardiotoxicity in the heavily pretreated pediatric patient population. This was achieved with 5-day 250 mg/m^2/day Bisantrene with 1,000 mg/m^2/ Ara-C given twice daily for 5-days. To evaluate the potential cardioprotection of Bisantrene in combination with Ara-C, I think it is important for investors to first realise how pretreated this patient population was. Here is a summary of prior therapy for the patients included into the study:
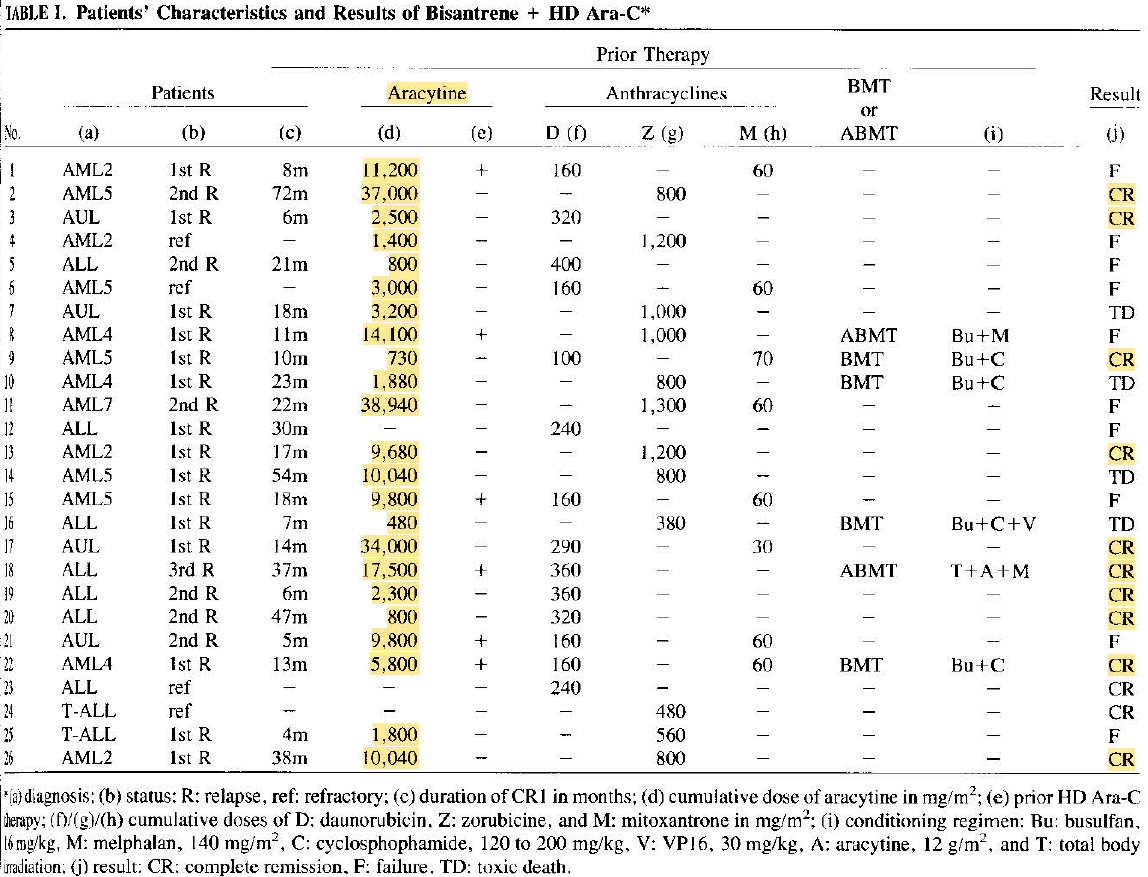
All patients had received one (17 patients), two (6 patients), or three (3 patients) different anthracyclines. Fourteen patients had been treated with daunorubicin at a mean cumulative dose of 245 mg/m², with a range from 160 to 400 mg/m². Twelve patients received zorubicin at a mean cumulative dose of 860 mg/m², ranging from 380 to 1300 mg/m². Eight patients had been treated with mitoxantrone, at a mean cumulative dose of 58 mg/m², ranging from 30 to 70 mg/m². Four patients (specifically patients 1, 11, 15, 22) received amsacrine, with a cumulative dose ranging from 300 to 450 mg/m². Twenty-three patients had received cytarabine (aracytine) with a mean cumulative dose of 9860 mg/m². Ara-C was administered using various schedules: a standard dose (100 to 200 mg/m²/day in continuous infusion) to 16 patients, a low dose (25 to 30 mg/m² twice a day subcutaneously) to 13 patients, and a high dose (1 to 2 mg/m² twice a day intravenously) to 6 patients.
There is some evidence to suggest that high dose Ara-C can cause elements of cardiotoxicity, though it is certainly not as well established or potent as other cardiotoxic agents.
https://www.sciencedirect.com/science/article/abs/pii/014521269400123R
https://www.sciencedirect.com/science/article/pii/S0923753420325370
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9681701/
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7956511/
https://onlinelibrary.wiley.com/doi/pdf/10.1002/ajh.2830410219
https://jamanetwork.com/journals/jamainternalmedicine/article-abstract/604846
If HD Ara-C was even marginally cardiotoxic, I suspect the combination of heavily pretreated, heart damaged patients, very mild cardiotoxicity from HD Ara-C, and FTO inhibition from Bisantrene may have synergised to produce some cardiotoxic effects. This may have then been rescued by the cardioprotective MoA’s of Bisantrene, given the dose of Bisantrene used in this study would well and truly be enough to provide significant cardioprotection. This interpretation of the data is flawed and filled with limitations, and it is impossible to know what was specifically happening at the biological level in these patients, but the fact that there was no cardiotoxicity is unequivocal.
Something that I have overlooked is that 88.5% of patients included in this study had received Ara-C and were refractory (resistant) to it. Refractory AML indicates that despite treatment, the leukemia cells continue to persist or multiply. This resistance can occur because the cancer cells develop mechanisms to evade the drug’s effects, often leading to poor clinical outcomes. Below is a table from that paper highlighting the doses of chemotherapy each patient had received prio to the study.
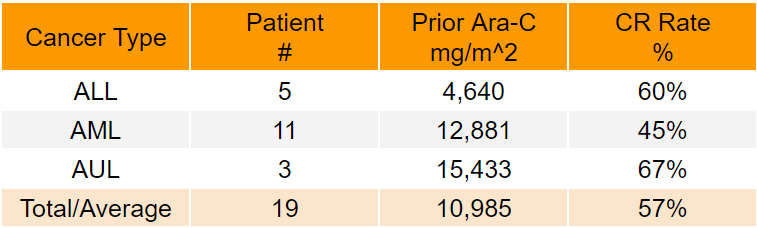
Excluding patients who had not received prior Ara-C (n=3) and who died due to infection and tumor lysis syndrome (n=4), Bisantrene in combination with Ara-C demonstrates an overall 57% CR rate (ALL 3/5 CR=60%, AML 5/11 CR=45%, and AUL 2/3 CR=67%). Subtypes of ALL, AUL, and AML were included into the same parent grouping.
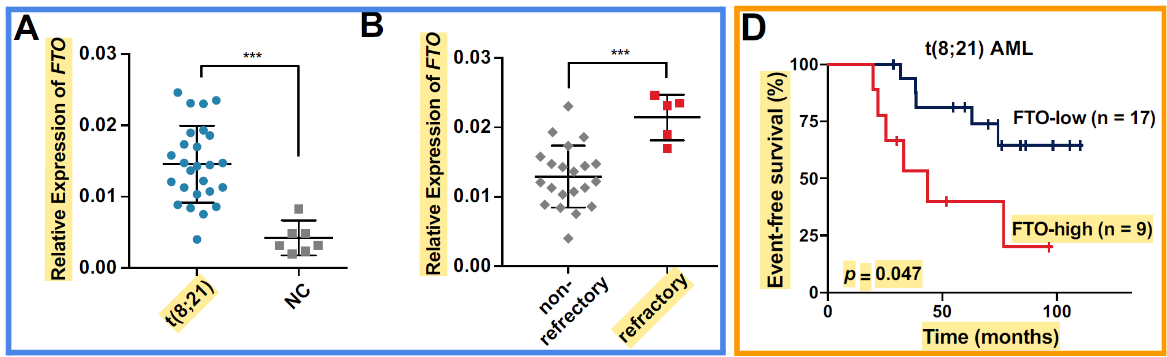
While the biological systems driving the excellent responses in this phase II paper were queried but not understood, recent research that has been replicated by two independent research groups highlights the role of FTO in AML refractory to Ara-C treatment. It is essential that investors understand this data and how it relates to the clinical responses seen in the P2 pediatric trial.
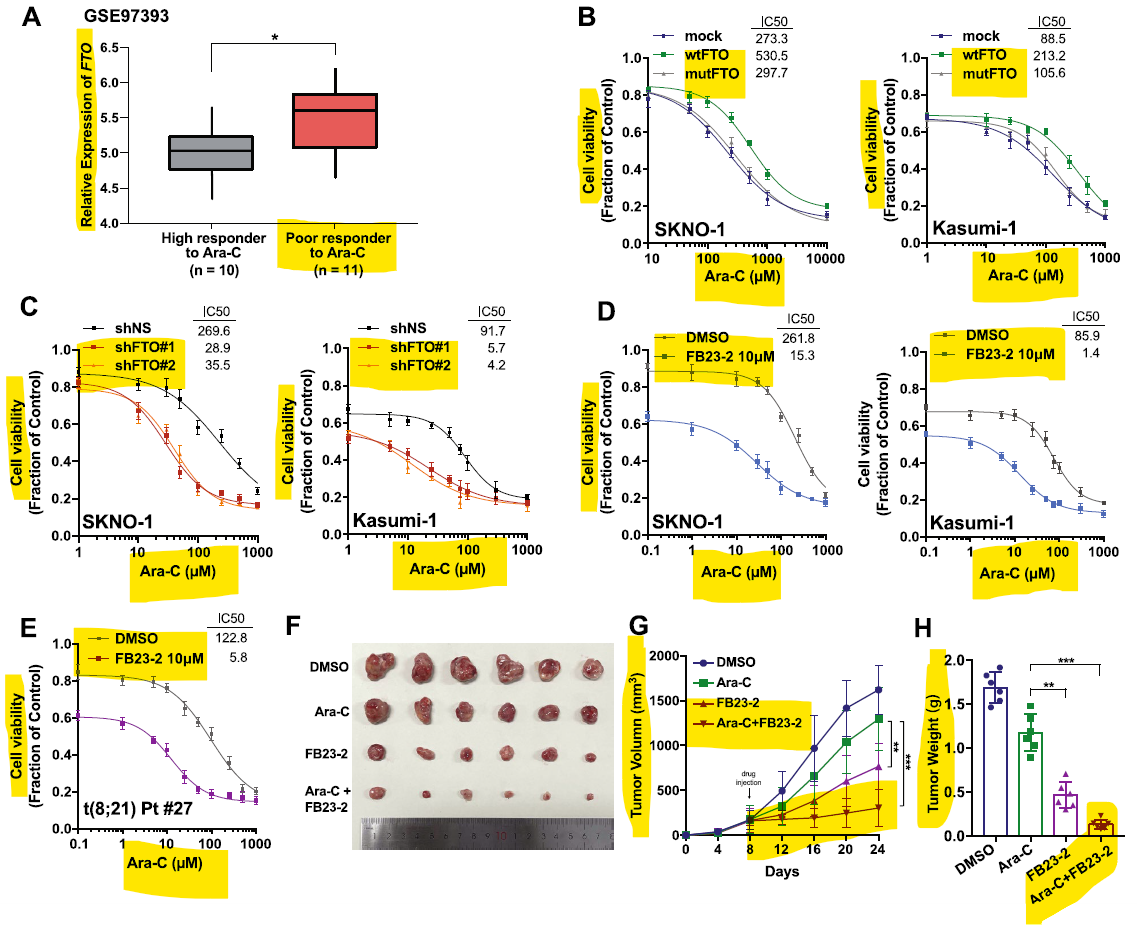
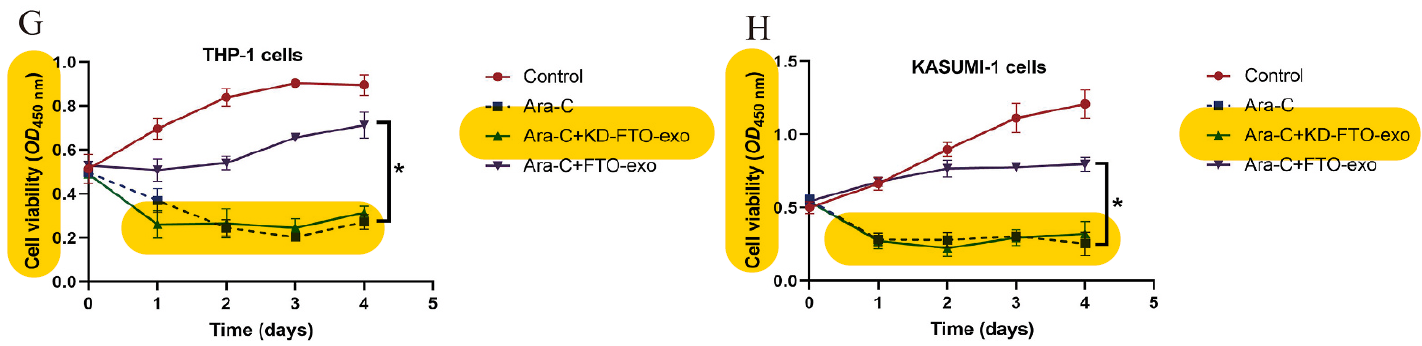
Zhou et al. (2024) demonstrates that FTO is overexpressed in AML and refractory AML (blue border) with progression free survival smallest in the FTO high groups (orange border). Poor responders to Ara-C treatment had significantly higher FTO levels, and FTO inhibition/knockdown reversed Ara-C resistance in vitro and in vivo to sensitize AML cells to Ara-C treatment (green border). Look specifically at the bottom right hand corner of the green border - in an Ara-C resistant AML in vivo model, an FTO inhibitor resensitizes Ara-C resistant AML cells and then synergises to effectively kill cancer better than single agent FTO inhibitor or Ara-C. Kou et al. (2024) repeated these findings by demonstrating forced FTO overexpression rendered AML cells resistant to Ara-C, and an FTO knockdown model in combination with Ara-C significantly decreased cell viability (purple border).
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10807068/pdf/40164_2024_Article_480.pdf
https://www.sciencedirect.com/science/article/abs/pii/S0013935123025872
Based on many lines of evidence, it is my belief that Bisantrene in combination with Ara-C achieved a 57% complete response rate in heavily pretreated, relapsed and refractory AML, ALL, and AUL patients with no clinically relevant cardiotoxicity due to FTO inhibition of cancer alongside cardioprotective mechanisms within heart cardiomyocytes. This would mark the first ever recorded successful synergy trial combining an FTO inhibitor with chemotherapy, where an FTO inhibitor resensitizes refractory cancer to treatment.
Conclusion
The role of m6A mRNA epitranscriptomics in the treatment of cancer is evolving rapidly. The data collected and interpreted within this report investigated the role of FTO in cardiotoxicity, and specifically the potential synergism between FTO inhibitors and cardiotoxic drugs to damage HCM. If this data drives meaningful cardiotoxicity in patients receiving combination FTO inhibitor and cardiotoxic agent, it will isolate Bisantrene as one of the only FTO inhibitors for use in patients alongside cardiotoxic agents (of which, there are many) - driving clear implications for the commercial opportunities for Bisantrene. We are in the infancy of understanding the role FTO inhibitors can play clinically and commercially, but cardiotoxicity synergy may be a significant hurdle that future developers of FTO inhibitors have to overcome. While there is enough clinical data to safely state that Bisantrene’s cardioprotective MoA(‘s?) are efficacious enough to overcome FTO inhibition in the heart, the current data for Bisantrene in combination with chemotherapy is excellent but is still developing for cardiotoxic agents. The fact remains that Bisantrene in combination with marginally cardiotoxic agents in heavily pretreated patients produced no clinical cardiotoxic events. Bisantrene in combination with anthracyclines will be an excellent test of the cardioprotective effects, and I personally am very confident in the potential of the drug to treat cancer while also providing cardioprotective benefits. This is bolstered by refractory cancers demonstrating acute sensitivity when treated with a potent inhibitor of the FTO protein, while preclinical work proves the mechanism for this effect - FTO inhibition abolishing chemoresistance. I can’t even begin to imagine what the percentage chance of finding another Bisantrene would be. The most potent inhibitor of a protein expressed in 30+ cancer types that controls cellular function and linked to the root cause of cancer as well as cardioprotective mechanisms that overcome FTO-inhibition + chemotherapy induced cardiotoxicity - it’s just unheard of. What may be more more unheard of is having access to a large clinical history that enables investors to understand how the drug was functioning 40 years ago and evaluate clinical risk.
I’d recommend sitting down and putting your reading glasses on...










Add RAC (ASX) to my watchlist
 (20min delay) (20min delay)
|
|||||
|
Last
$1.69 |
Change
0.000(0.00%) |
Mkt cap ! $288.0M | |||
| Open | High | Low | Value | Volume |
| $1.66 | $1.69 | $1.57 | $387.6K | 237.1K |
Buyers (Bids)
| No. | Vol. | Price($) |
|---|---|---|
| 1 | 807 | $1.63 |
Sellers (Offers)
| Price($) | Vol. | No. |
|---|---|---|
| $1.69 | 2376 | 1 |
View Market Depth
| Last trade - 16.10pm 04/10/2024 (20 minute delay) ? |
| RAC (ASX) Chart |