Title: Preclinical Advances of Bisantrene
Price Sensitive: Yes
Executive Summary:
Bisantrene has demonstrated promising efficacy in preclinical studies against various cancer types, coupled with significant cardioprotective effects when used in combination with other chemotherapeutic agents. This report synthesizes unannounced data from recent patent submissions and unpublished studies, detailing Bisantrene’s interaction with human cardiomyocytes, anthracycline and proteasome inhibitors, breast cancer cell viability, and cardioprotective properties in mouse models. The evidence highlights Bisantrene's clinical and commercial uniqueness as a potent anticancer agent with broad cardioprotective capabilities.
1. Cardioprotective Effects in Human Cardiomyocytes:
Bisantrene has mitigated the cardiotoxic effects of anthracyclines, such as daunorubicin and epirubicin, and the combined effects of doxorubicin and Herceptin. These findings suggest its potential to broadly shield against cardiotoxicity induced by both anthracyclines and monoclonal antibodies.
2. Interaction with Proteasome Inhibitors:
The drug extends its cardioprotective effects beyond anthracyclines, reducing cardiomyocyte toxicity in combinations with proteasome inhibitors like carfilzomib and bortezomib. This versatility underscores its potential integration into diverse chemotherapeutic regimens.
3. Impact on Breast Cancer Cell Viability:
Bisantrene exhibits dose-dependent cytotoxic effects on MDA-MB-231 breast cancer cells and enhances the cytotoxicity of doxorubicin and epirubicin, indicating synergistic interactions. Its mechanism appears distinct from known FTO inhibitors, suggesting a novel mode of cytotoxic synergy.
4. Cardioprotective Effects in Mouse Models:
Extensive mouse studies show that Bisantrene reduces histological cardiac fibrosis and improves cardiac function parameters like left ventricular diastolic function and cardiac output when combined with doxorubicin.
5. Comprehensive Analysis of Cardiac and Blood Parameters:
In mouse models, Bisantrene significantly lowers plasma triglyceride levels and creatine kinase-MB markers of cardiac damage, further evidencing its cardioprotective effects against chemotherapy-induced cardiotoxicity.
Market Opportunity:
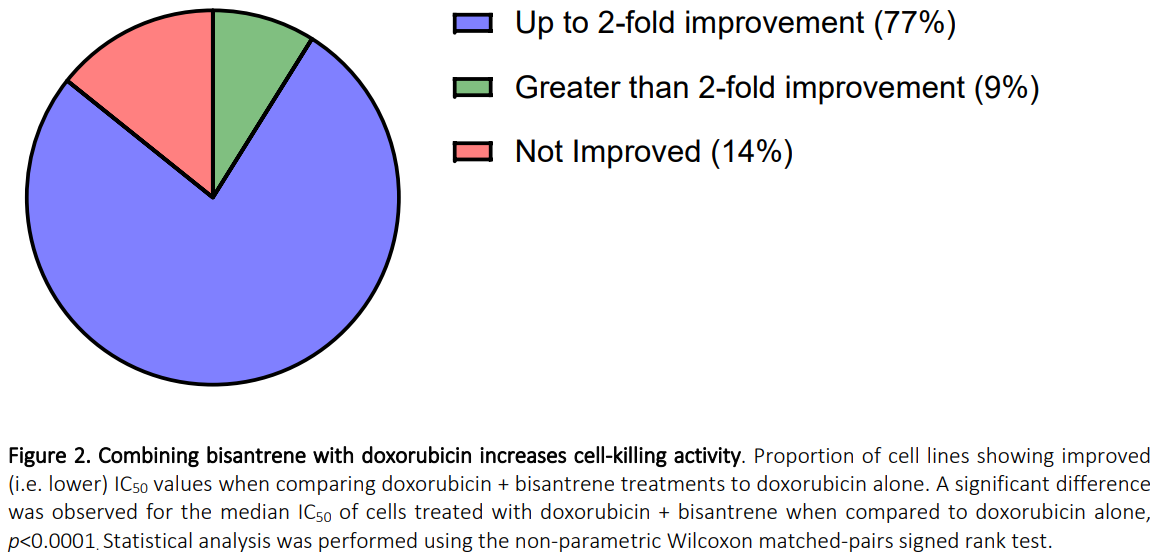
Given Bisantrene's demonstrated synergy with anthracyclines and proteasome inhibitors, along with its cardioprotective properties in combinations with doxorubicin and Herceptin, it holds substantial therapeutic potential. The broad applicability across various treatments suggests a mechanism of action that could enhance efficacy and reduce cardiotoxicity in a wide array of drug classes. Bisantrene has shown effective synergy with doxorubicin in 86% of tested cell lines across 15 cancer types and consistently provided cardioprotection, achieving a 100% success rate with cardiotoxic agents. This broad-spectrum efficacy highlights its potential as a versatile adjunct in cancer therapy, offering both enhanced anti-cancer activity and protection against drug-induced cardiac damage.
Investment Consideration:
Using conservative estimates, if Bisantrene captures even a fraction of the market based on its unique dual action, the financial projections could be substantial. The combined market potential for cancer treatment and cardioprotection opens a new frontier in oncological therapy, making Bisantrene a compelling investment with significant clinical and commercial prospects.
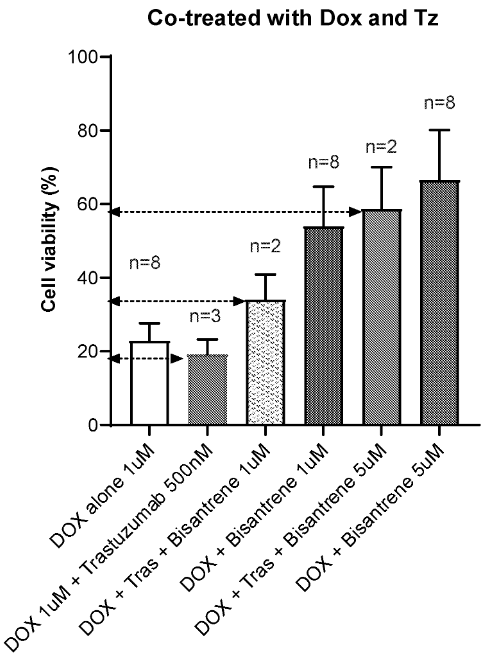
Bisantrene overcomes the combined cardiotoxicity of doxorubicin and herceptin
The figure illustrates the viability of HCMs when cultured under various conditions: 1 μM doxorubicin alone; 1 μM doxorubicin combined with 500 nM trastuzumab; 1 μM doxorubicin with both 500 nM trastuzumab and 1 μM bisantrene; 1 μM doxorubicin with 1 μM bisantrene; and 1 μM doxorubicin with 500 nM trastuzumab at two different concentrations of bisantrene (1 μM and 5 μM).
Bisantrene demonstrated a mitigating effect on the combined cardiotoxicity of doxorubicin and trastuzumab (each known for their cardiotoxic effects when used alone). As depicted below, cardiomyocytes cultured with both trastuzumab and doxorubicin exhibited lower viability compared to those cultured with doxorubicin alone. However, the introduction of bisantrene into the culture medium, regardless of whether it contained only doxorubicin or both doxorubicin and trastuzumab, led to a decreased reduction in cell viability. Notably, the inclusion of 5 μM bisantrene resulted in a smaller difference in viability compared to using 1 μM bisantrene, highlighting its effectiveness at higher concentrations.
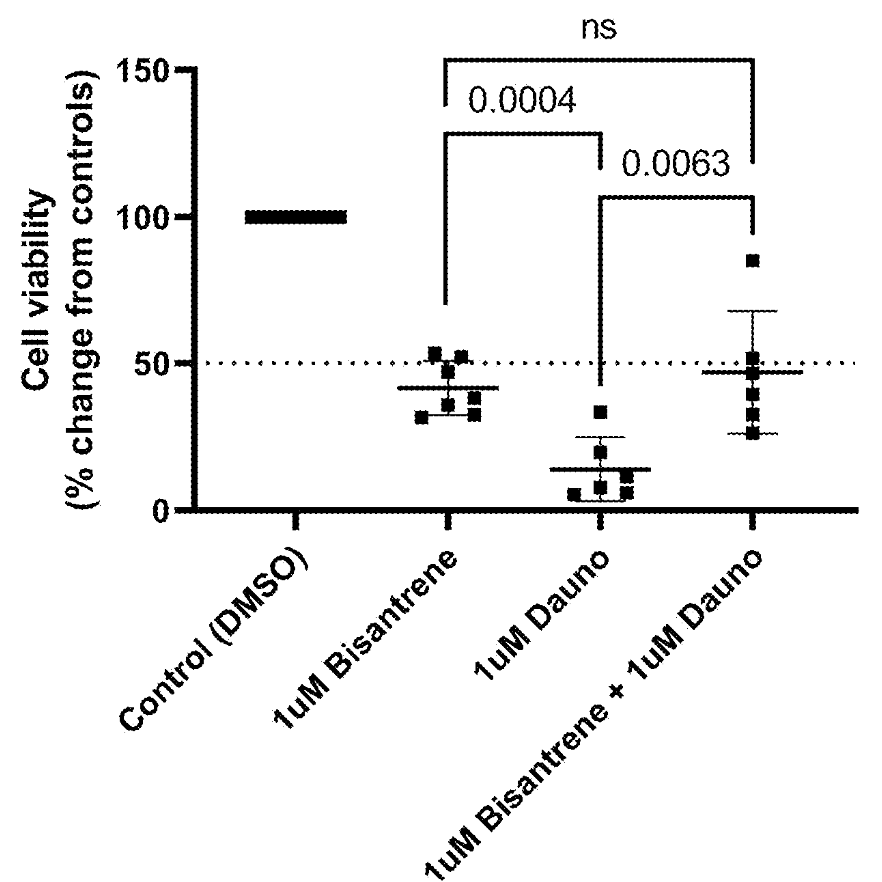
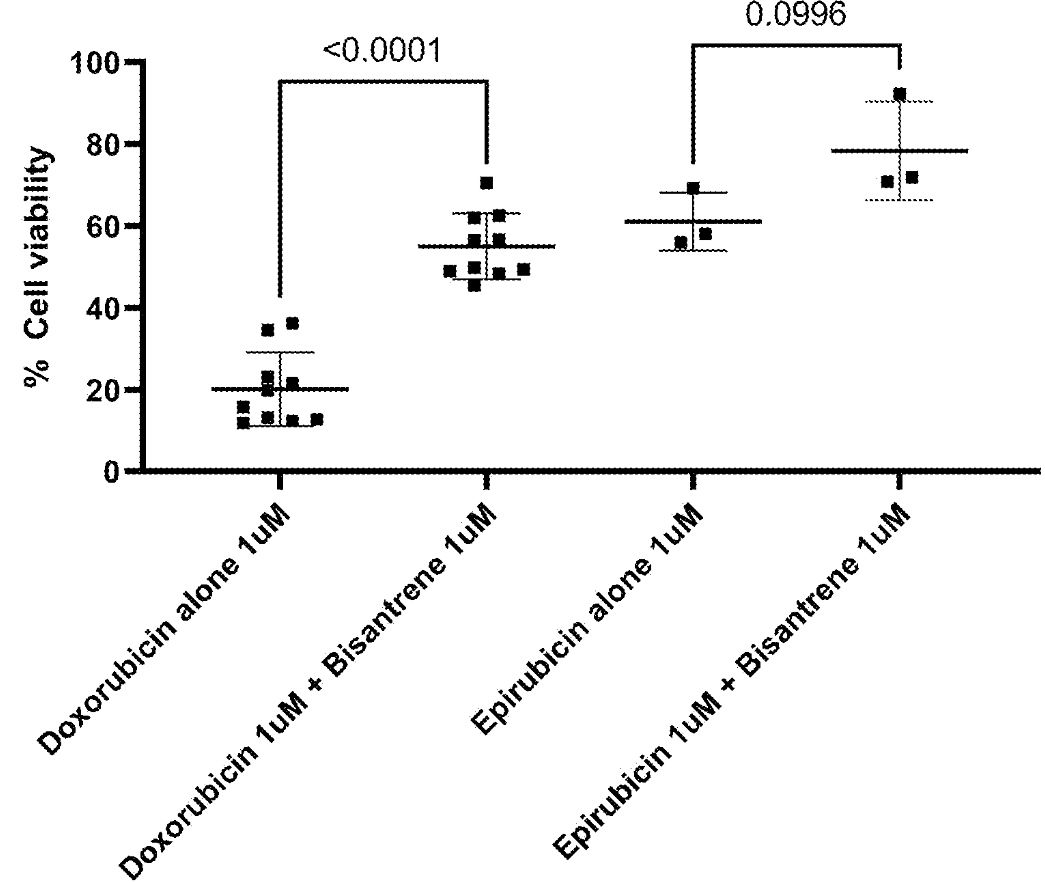
Bisantrene overcomes the cardiotoxicity of other anthracyclinesAs seen below, HCM cell viability is illustrated when cultured in the presence of 1 μM bisantrene, 1 μM daunorubicin, or a combination of both for 72 hours (orange). Similarly, the blue figure displays the viability of HCMs when cultured with 1 μM doxorubicin alone, 1 μM doxorubicin with 1 μM bisantrene, 1 μM epirubicin alone, or 1 μM epirubicin with 1 μM bisantrene for the same duration.
These results demonstrate the cardiotoxicity rescue effects of bisantrene on cardiomyocytes, extending to the anthracycline daunorubicin when both agents are administered at 1 μM. Similarly, a trend toward statistical significance is observed for the coadministration of epirubicin and bisantrene at 1 μM. These observations support that the cardioprotective effects of bisantrene are general across the anthracycline class of chemotherapeutic agents.
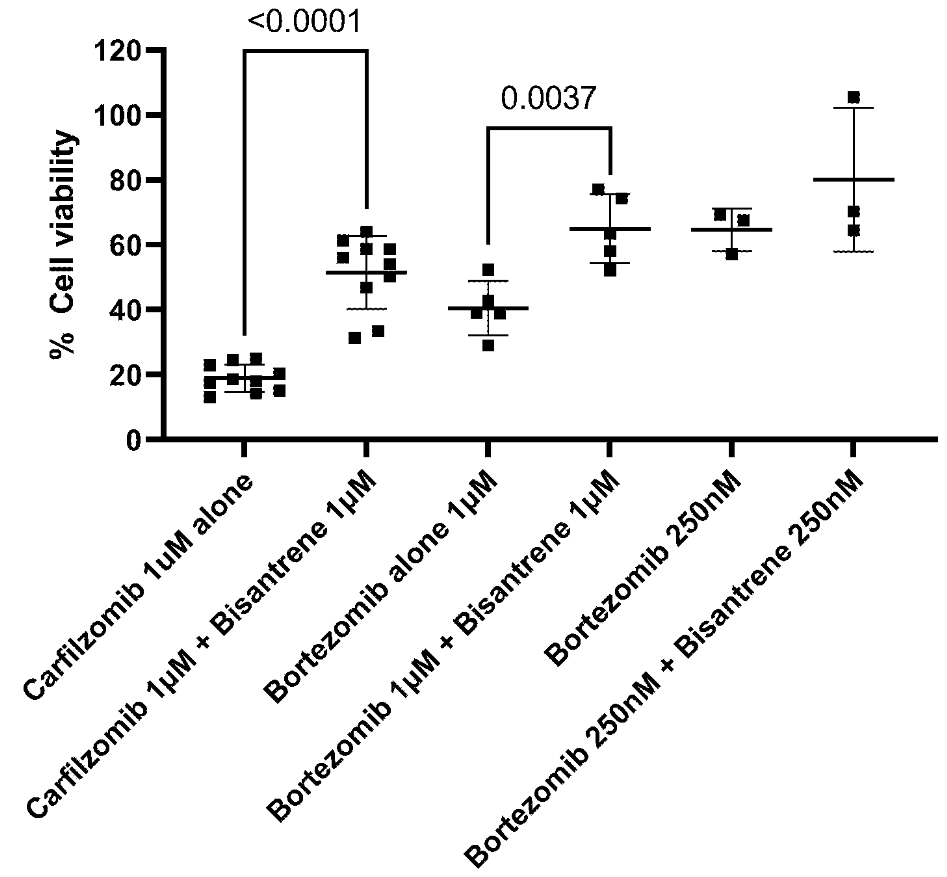
Bisantrene overcomes the cardiotoxicity of proteasome inhibitors
As seen below, HCM cell viability is depicted when cultured with approved proteasome inhibitors alone, or in combination with 1 μM bisantrene at various concentrations for 72 hours.
This illustration further demonstrates that the cardioprotective effects of bisantrene are not exclusive to the anthracycline class. Significant rescue of cardiomyocyte toxicity is observed with both the irreversible proteasome inhibitor, carfilzomib, and the reversible inhibitor, bortezomib, when each is coadministered with bisantrene.
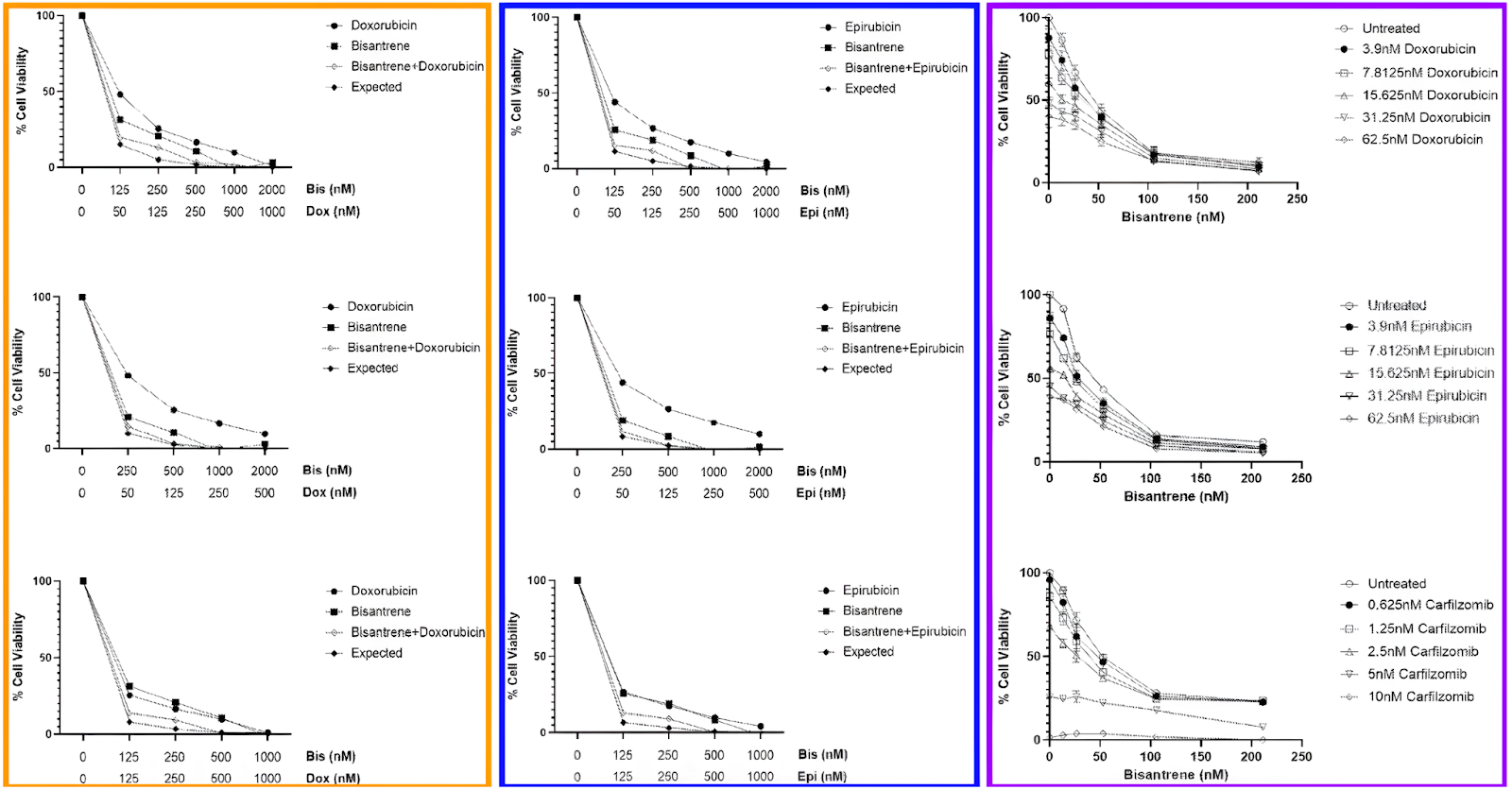
Bisantrene demonstrates consistent synergy with anthracyclines and proteasome inhibitors in breast cancer cell line
The following figure presents a comprehensive analysis of MDA-MB-231 breast cancer cell viability under various treatment regimens. The diagram with the orange border illustrates the cell viability when exposed to varying concentrations of bisantrene and doxorubicin, either alone or in combination. This chart shows a range of conditions from no treatment to maximum dosage, highlighting the expected additive effects of these drugs when used together at different concentrations.
In the diagram with the blue border, a similar analysis is conducted using bisantrene and epirubicin. Here too, the cells are exposed to varying concentrations of both drugs, alone and in combination, to observe potential additive effects. This setup mirrors the first but swaps doxorubicin with epirubicin, allowing for a direct comparison of the impact of these two different anthracyclines when used in conjunction with bisantrene.
Finally, the diagram with the purple border shifts focus slightly by examining the effects of bisantrene combined with multiple concentrations of doxorubicin, epirubicin, and carfilzomib, a proteasome inhibitor. This detailed exploration provides insight into how bisantrene interacts not only with anthracyclines but also with other types of chemotherapeutic agents, demonstrating its influence across a broader range of combinations and concentrations.
When evaluated with MDA-MB-231 breast cancer cells, the concentration-dependent toxicity of bisantrene was confirmed once again. Moreover, the effects of bisantrene were found to be at least additive, if not synergistic, when combined with doxorubicin, epirubicin, or carfilzomib, according to a Webb synergy analysis. This enhancement in combined drug activity was particularly notable at lower drug concentrations, as illustrated in the accompanying figures.
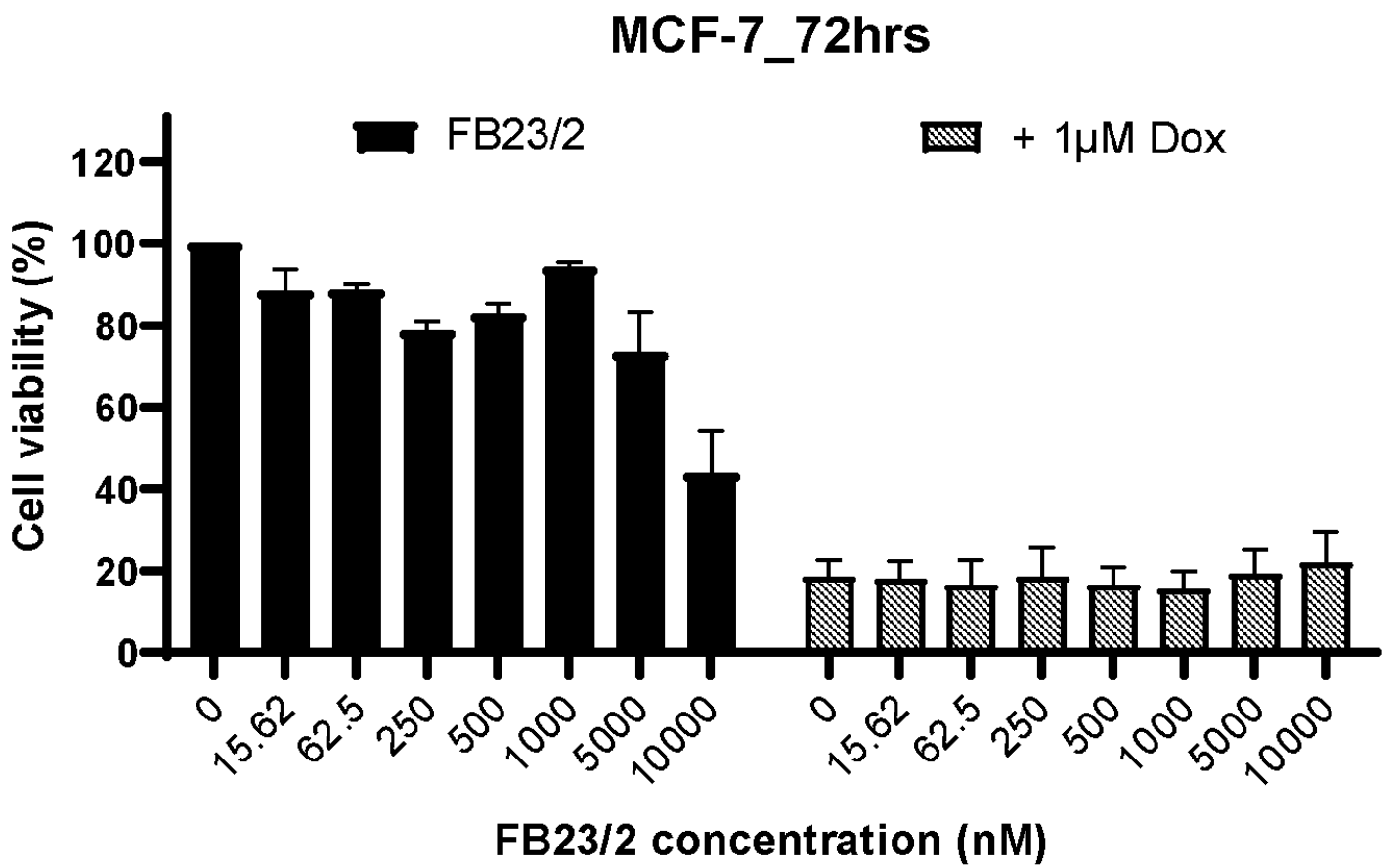
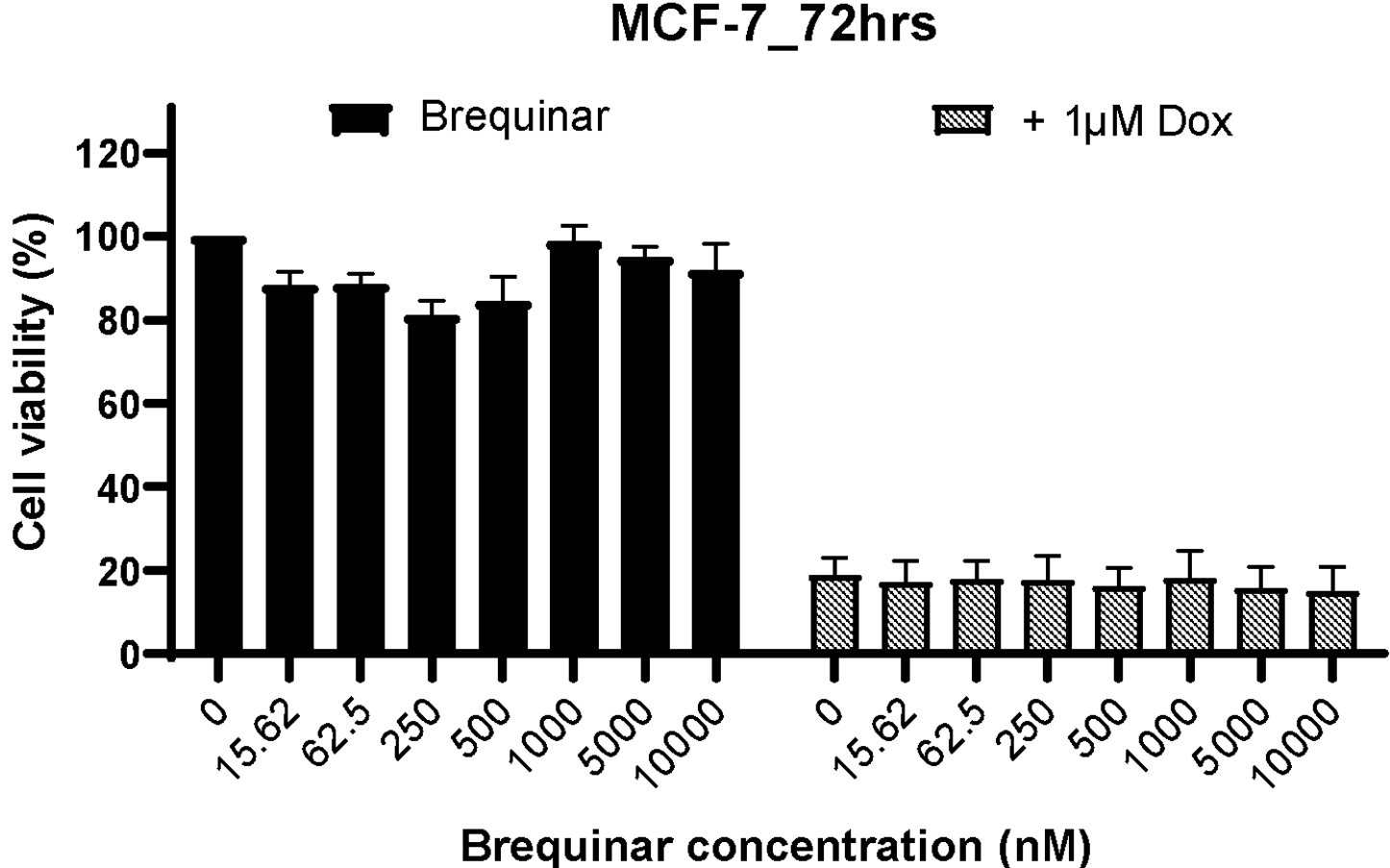
FTO inhibitors do not synergise with doxorubicin in breast cancer cell line
The following figures illustrate the viability of MCF-7 breast cancer cells when exposed to the FTO inhibitors FB23/2 (green) and brequinar (blue), either alone or in combination with 1 μM doxorubicin over a 72-hour period.
MCF-7 breast cancer cells and H929 multiple myeloma cells were also tested with brequinar and FB23/2, both alone and in conjunction with doxorubicin, to evaluate whether these FTO inhibitors could enhance the loss of cancer cell viability when used with doxorubicin. The results demonstrated that neither brequinar nor FB23/2, even at concentrations up to 10 μM, increased the loss of viability in MCF-7 breast cancer cells or H929 multiple myeloma cells treated with 1 μM doxorubicin for up to 72 hours.
The results indicate that the enhanced toxic effects observed between bisantrene and doxorubicin or epirubicin over 72 hours on MCF7, MDA-MB-231 breast cancer cells, and H929 multiple myeloma cells may not be attributable to the FTO inhibitor activity of bisantrene.
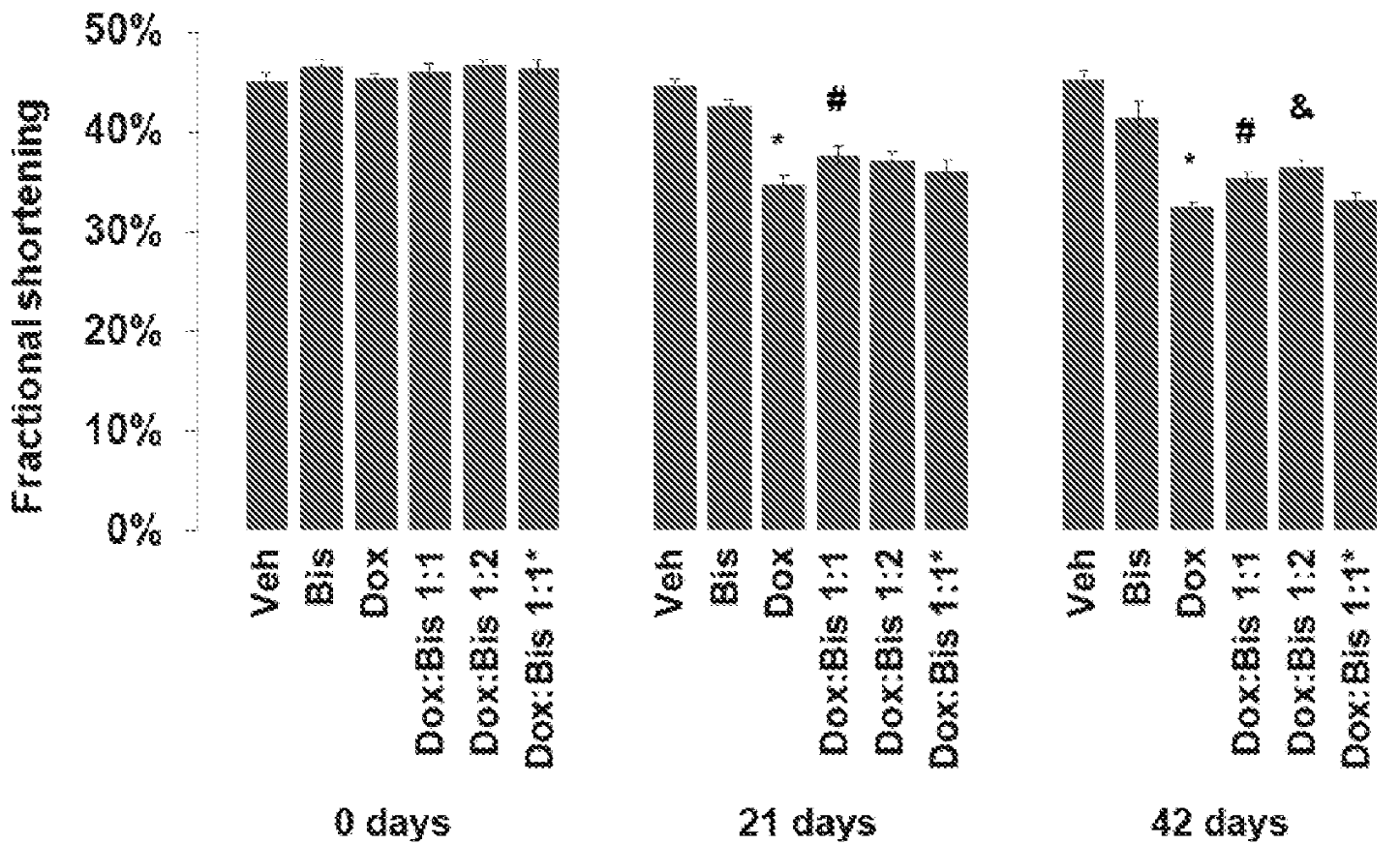
Bisantrene consistently alleviates doxorubicin-related cardiotoxic effects
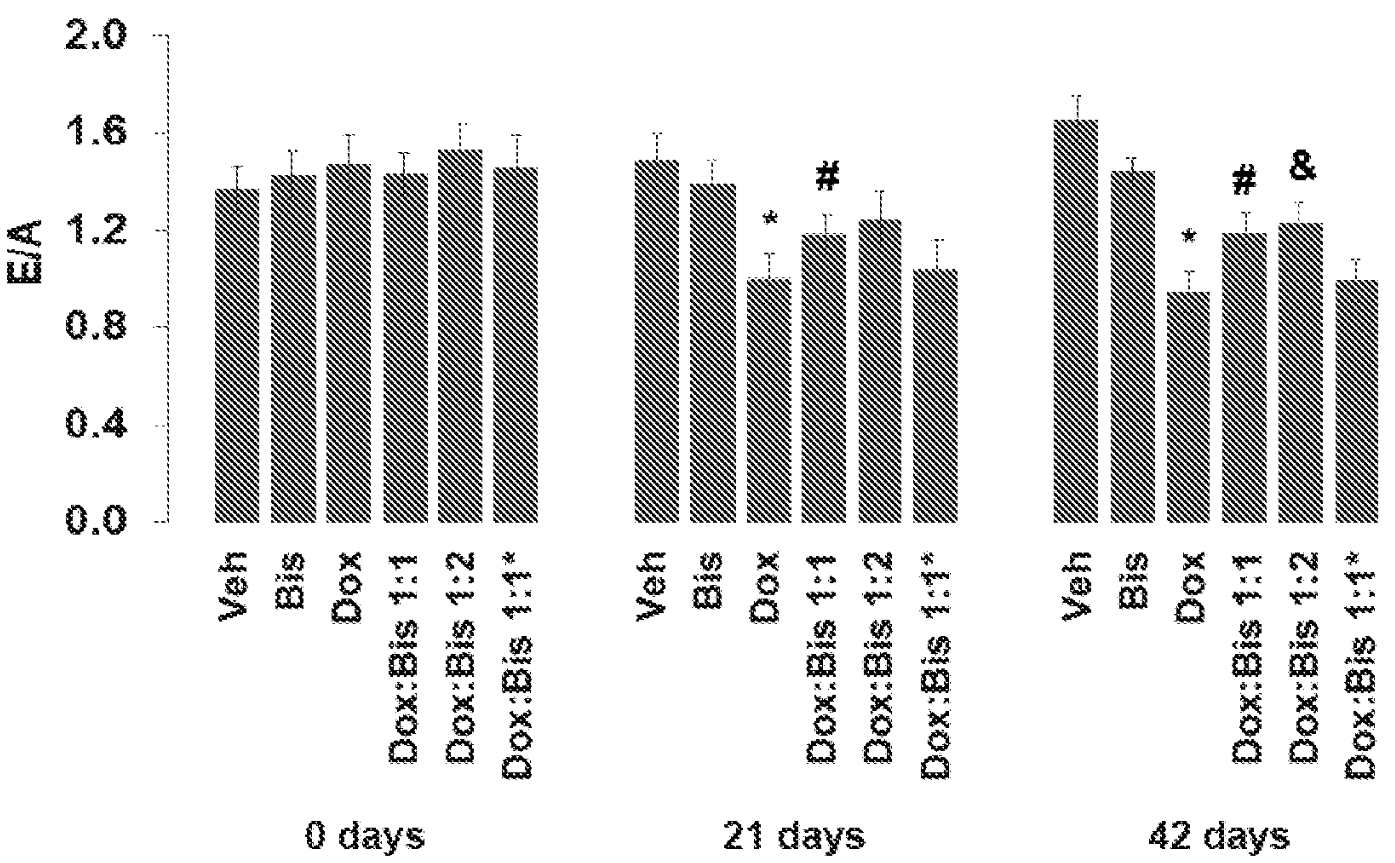
The below presents the following observations: (yellow) the impact of bisantrene on left ventricular shortening in mice, administered either alone or in combination with doxorubicin; and (red) the influence of bisantrene on the heart E/A ratio in mice under similar conditions. The specific dosages tested included vehicle alone; 7.33 mg/kg of bisantrene once weekly for four weeks alone; 5 mg/kg of doxorubicin once weekly for four weeks alone; a combination of 5 mg/kg doxorubicin with 3.67 mg/kg bisantrene (Dox:Bis 1:1) once weekly for four weeks; a combination of 5 mg/kg doxorubicin with 7.33 mg/kg bisantrene (Dox:Bis 1:2) once weekly for four weeks; and a combination of 4 mg/kg doxorubicin with 5.65 mg/kg bisantrene (Dox:Bis 80:20) once weekly for four weeks. Notable findings indicated with statistical markers showed that doxorubicin combined with vehicle significantly impacted heart function by Days 21 and 42 (*: p < 0.001), while combinations of doxorubicin with bisantrene at different ratios showed varying degrees of mitigation of these effects (#: p < 0.05 for Dox+Bis 1:1 and &: p < 0.01 or p <0.05 for Dox+Bis 1:2 depending on the measure and day).
From these results, it appears that although bisantrene alone at 7.33 mg/kg (approximately 22 mg/m2) per dose suggests a mild deleterious impact on left ventricular fractional shortening and heart E/A ratio, the significant cardiotoxic effects of doxorubicin observed in vivo were considerably alleviated when co-administered with bisantrene. Notably, the protection was more pronounced with the higher bisantrene ratio (Dox+Bis 1:2), indicating an optimal protective effect at this ratio, with a less marked effect observed in the Dox+Bis 80:20 treatment scenario.
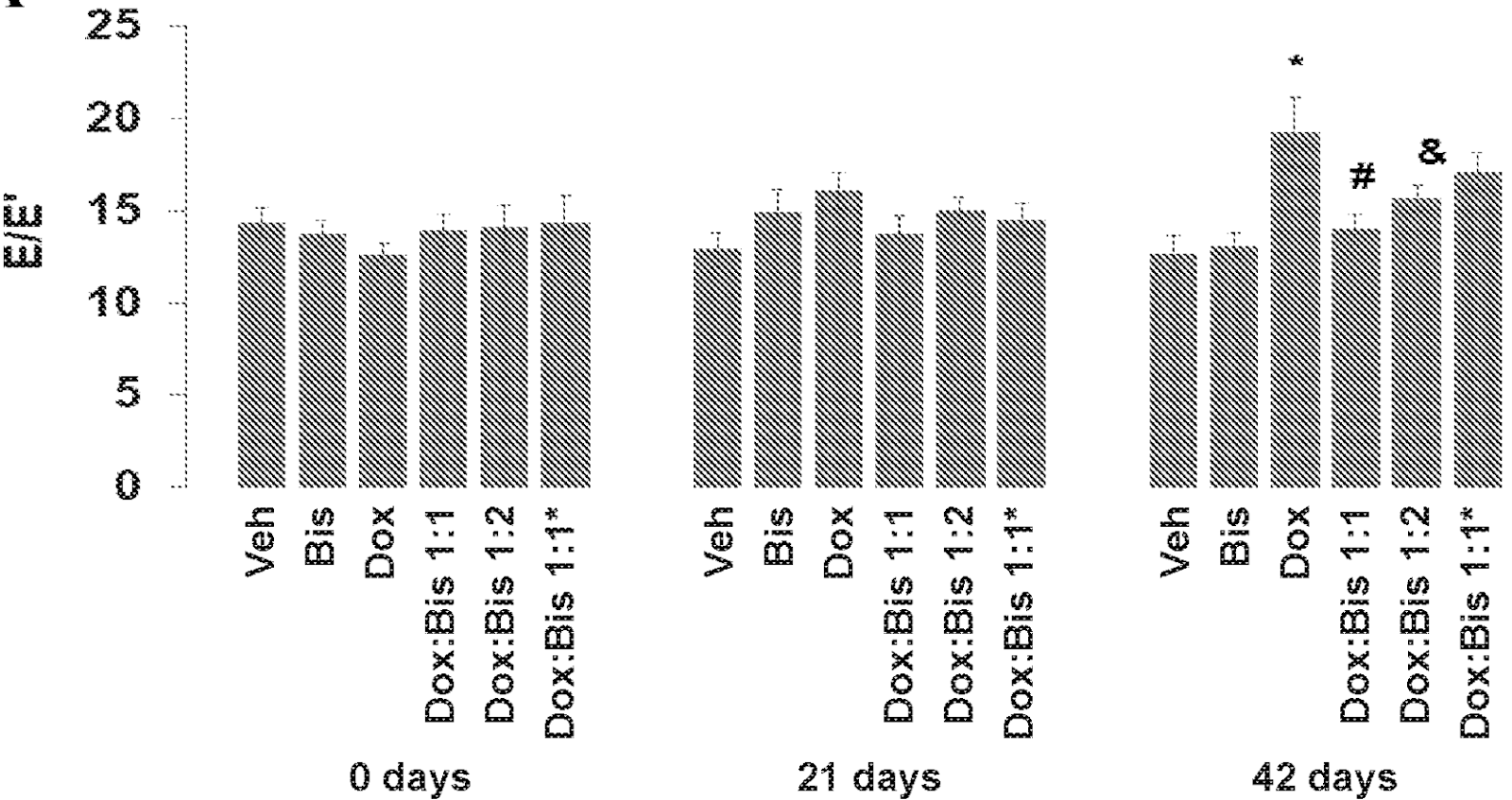
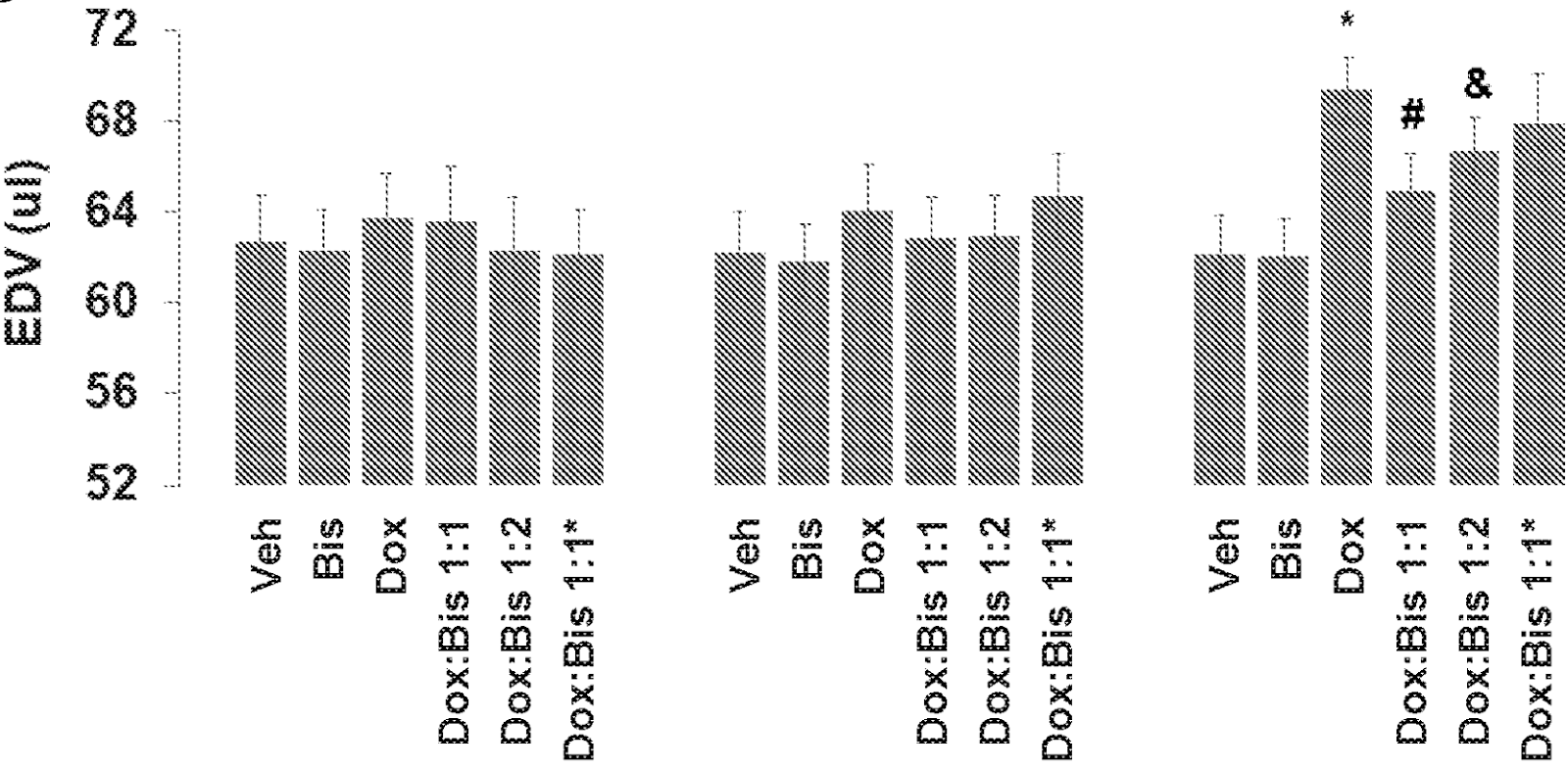
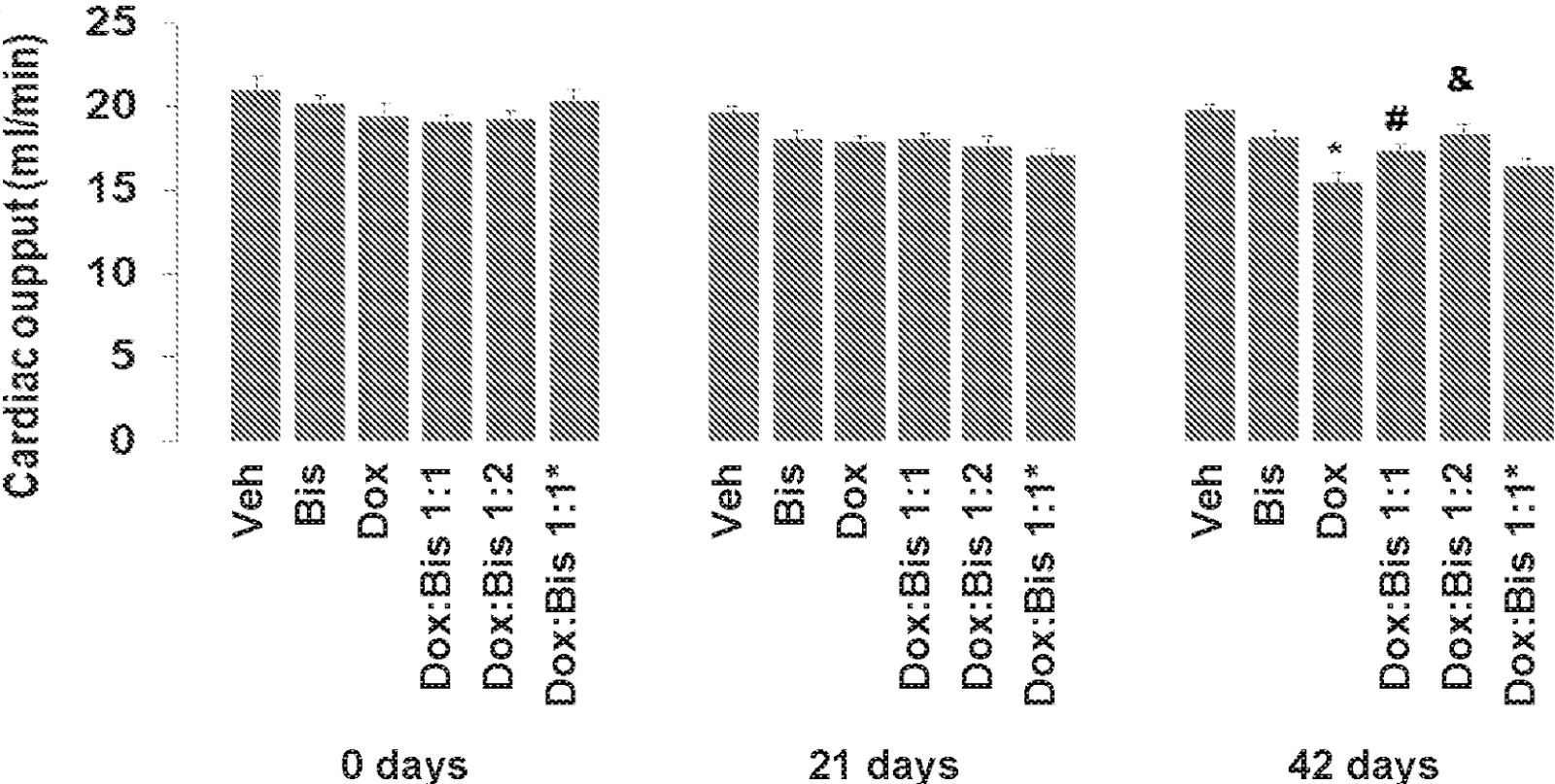
The below illustrates the impact of bisantrene on various cardiac functions in mice, administered either alone or in combination with doxorubicin. The figure details the effects on (pink) left ventricular diastolic function, (brown) left ventricular dilatation, and (red) cardiac output. The specific regimens tested include vehicle alone; 7.33 mg/kg bisantrene administered once weekly for four weeks; 5 mg/kg doxorubicin once weekly for four weeks; combinations of 5 mg/kg doxorubicin with 3.67 mg/kg bisantrene (Dox:Bis 1:1), 7.33 mg/kg bisantrene (Dox:Bis 1:2), and a further reduced dose ratio of 4 mg/kg doxorubicin to 5.65 mg/kg bisantrene (Dox:Bis 80:20), each administered once weekly for four weeks. Notable findings indicated significant differences where doxorubicin combined with vehicle markedly affected cardiac function by Day 42 (*: p < 0.01). Differences in treatment outcomes were also highlighted where the Dox:Bis 1:1 combination showed a protective effect against doxorubicin's cardiotoxicity by Day 42, with statistical significance in left ventricular functions and cardiac output (#: p < 0.05 in A and B; p < 0.01 in C). The Dox:Bis 1:2 combination displayed variable significance across the measurements (&: ranging from p < 0.09 to p < 0.01).
The results from the below suggest that while bisantrene alone at 7.33 mg/kg (approximately 22 mg/m2) might have mild deleterious effects on cardiac functions, these are not significant. Doxorubicin, on the other hand, showed notable cardiotoxic effects at 42 days post-treatment initiation. The combination of bisantrene and doxorubicin, particularly at a 1:1 molar ratio, effectively mitigated these effects, particularly in left ventricular diastolic function and dilatation, compared to higher bisantrene dosages. For cardiac output, the Dox:Bis 1:2 treatment showed slightly greater mitigation of cardiotoxicity compared to the Dox:Bis 1:1 treatment, with the least effect observed in the treatment approximating an 80% dose of the 1:2 ratio.
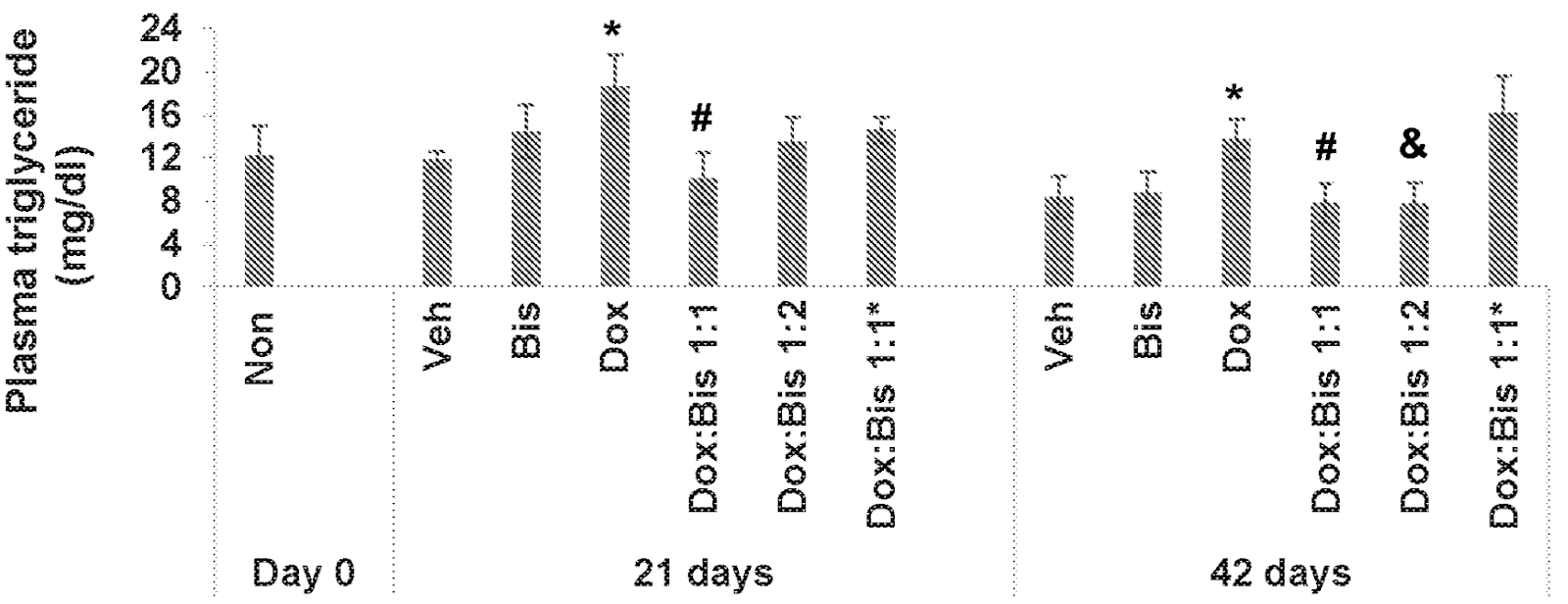
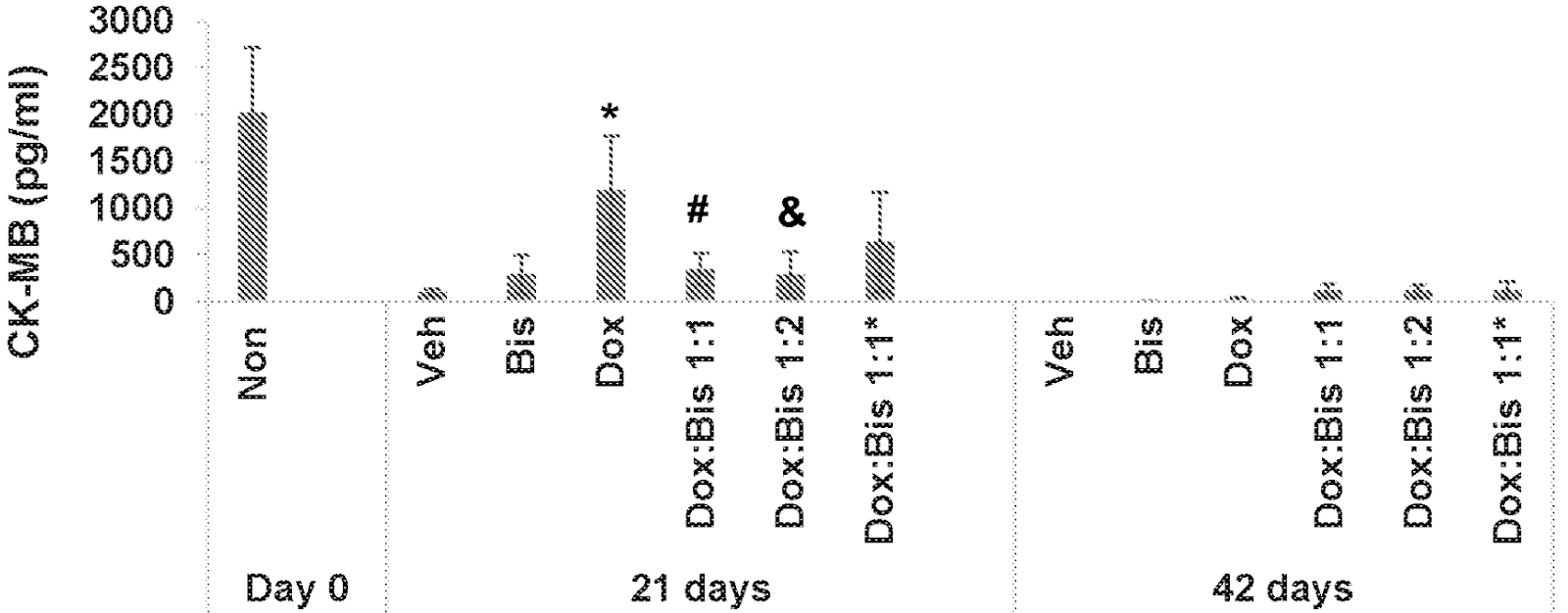
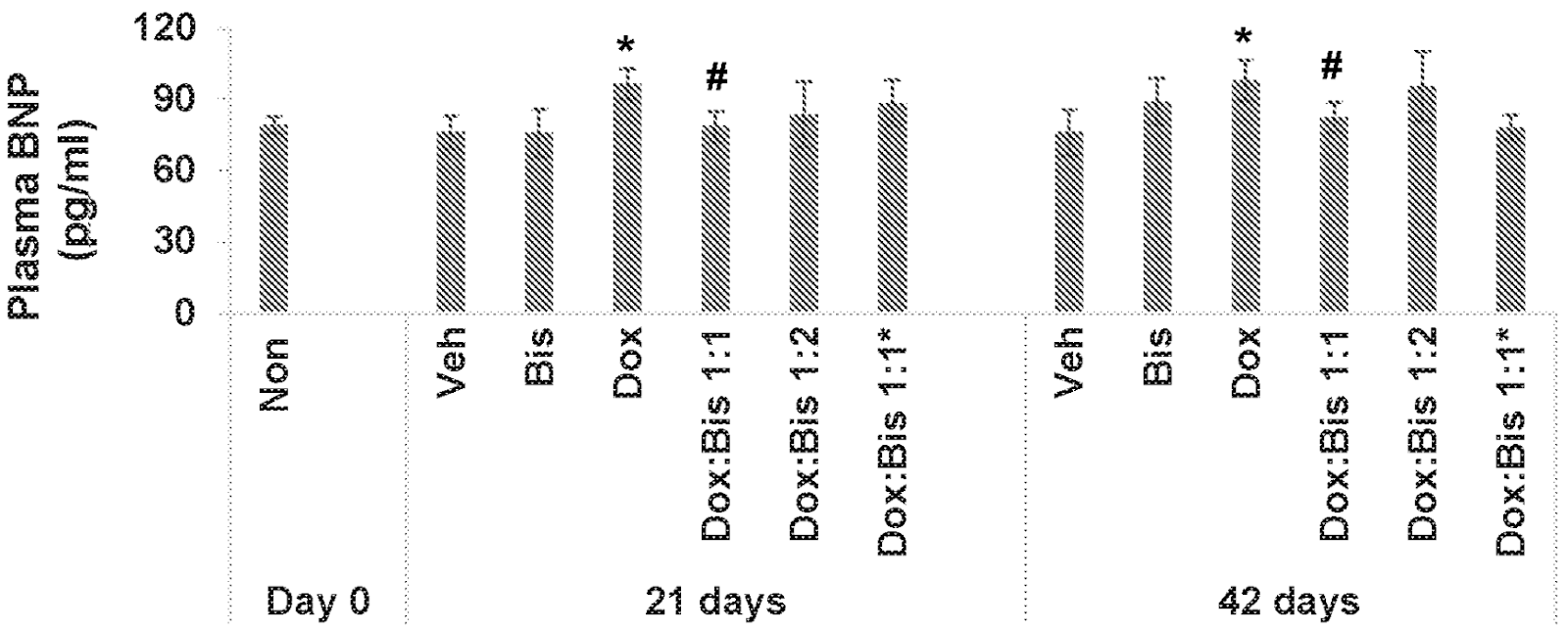
Below presents the impact of bisantrene on various cardiac and blood parameters in mice, both alone and in combination with doxorubicin. The figure details the effects on (green) plasma triglyceride levels, (orange) blood creatine kinase-MB (CK-MB), and (purple) plasma brain natriuretic peptide (BNP).
Plasma Triglyceride Levels (A): Bisantrene alone showed a slight but non-significant increase in plasma triglycerides at day 21, with no changes at day 42 compared to the vehicle-only control. However, doxorubicin treatment alone significantly elevated triglyceride levels at both day 21 and day 42. When bisantrene was co-administered with doxorubicin in the Dox:Bis ratios of 1:1 and 1:2, there was a significant reduction in the doxorubicin-induced increase in triglycerides at both time points, with a diminished effect observed in the Dox:Bis 80% of 1:2 treatment.
Blood Creatine Kinase-MB (B): Administration of bisantrene and doxorubicin significantly moderated the increase in CK-MB levels induced by doxorubicin alone at day 21. The protective effects were most pronounced in the Dox:Bis 1:1 and 1:2 treatments, maintaining CK-MB levels close to those of the vehicle control, with no significant changes observed at day 42.
Plasma Brain Natriuretic Peptide (C): Similar patterns were observed with BNP levels, where bisantrene co-administration mitigated the rise induced by doxorubicin, especially evident in the Dox:Bis 1:1 treatment at both day 21 and day 42. The results for the Dox:Bis 1:2 ratio were not significantly different from doxorubicin alone at these time points.
Additional Findings: No significant effects were observed on plasma LDH levels, eosinophil, neutrophil, basophil, lymphocyte levels or viabilities, hematocrit or hemoglobin levels, mean corpuscular volume, platelet counts, red or white blood cell counts, or the heart weight/body weight ratio when bisantrene was co-administered with doxorubicin.
This comprehensive data from the information below highlights the potential of bisantrene to reduce some of the cardiotoxic effects induced by doxorubicin, particularly affecting triglyceride and CK-MB levels, with varying efficacy depending on the ratio of doxorubicin to bisantrene.
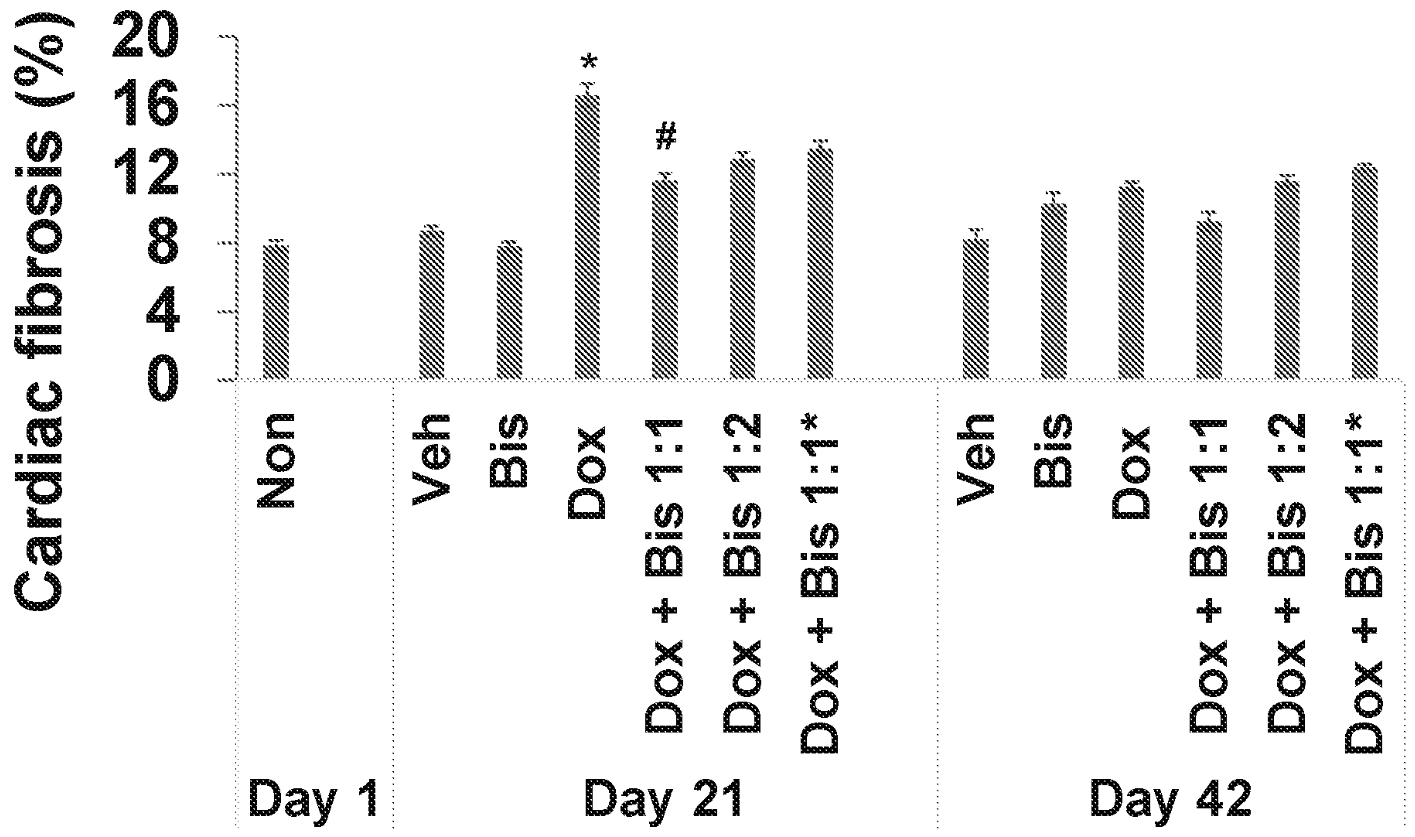
The figure below illustrates the impact of bisantrene on histological cardiac fibrosis in mice, administered either alone or in combination with doxorubicin. The findings show significant reductions in fibrosis when bisantrene is co-administered with doxorubicin at a 1:1 molar ratio (*: p < 0.01, Dox+Vehicle vs. Vehicle at Day 21; #: p < 0.05, Dox+Bis 1:1 vs. Dox+Vehicle at Day 21).
The results confirm that bisantrene, when combined with doxorubicin at a 1:1 molar ratio, substantially decreases histologic cardiac fibrosis by Day 21 compared to mice receiving doxorubicin alone. This outcome aligns with functional echocardiographic data and blood biomarker results, underscoring bisantrene's capability to reduce a key structural marker of anthracycline-induced cardiac damage.
Additionally, bisantrene appears to enhance left ventricular systolic and diastolic function, and overall cardiac function (including cardiac output and brain natriuretic peptide levels) in doxorubicin-treated mice. These benefits are likely due to bisantrene’s role in mitigating early myocardial injury indicators such as CK-MB and cardiac fibrosis.
In this study, the protective effects of bisantrene were most pronounced when administered in a 1:1 ratio with doxorubicin (equivalent to about 3.67 mg/m2). However, the Dox:Bis 1:2 ratio also showed significant mitigation of certain doxorubicin-induced cardiotoxicity markers, though not as extensively as the 1:1 ratio.
Conclusion
These results cumulatively could be the sum of 3 - 4 price sensitive announcements, and expand the TAM for Bisantrene considerably. The cardioprotective effects for Bisantrene appear to be unrelated to the drug class, further opening the potential for cardiosynergy with multiple other drug classes known to be cardiotoxic. The cardioprotective mechanism for Bisantrene is currently unknown, but work is being done to understand the effects of Bisantrene in HCM when used in combination with cardiotoxic agents. It appears some of the cytotoxic synergistic effects of Bisantrene may not be related specifically to FTO, though further work is required to understand this mechanism. Since the secrets are soon to be revealed, Bisantrene is an increasingly exciting drug clinically and commercially.
OpportunityGiven the evidence that Bisantrene consistently shows cytotoxic synergy with anthracyclines and proteasome inhibitors, as well as providing cardioprotection in combination with doxorubicin and herceptin, anthracyclines, and proteasome inhibitors, it is reasonable for investors to be highly optimistic about its therapeutic potential. The mechanisms of action appear to be broad, contributing to synergy and cardioprotection across various treatments rather than being confined to a specific drug or class. This suggests that Bisantrene's effects are mediated through fundamental pathways that could enhance efficacy and reduce cardiotoxicity when combined with multiple drugs and drug classes. Notably, Bisantrene has shown synergy with doxorubicin in 86% of tested cell lines, encompassing 15 different cancer types. Furthermore, available data indicates that Bisantrene provides cardioprotection when used with any cardiotoxic agent, achieving a 100% success rate in these scenarios. This broad-spectrum efficacy highlights its potential as a versatile adjunct in cancer therapy, offering both enhanced anti-cancer activity and protection against drug-induced cardiac damage.
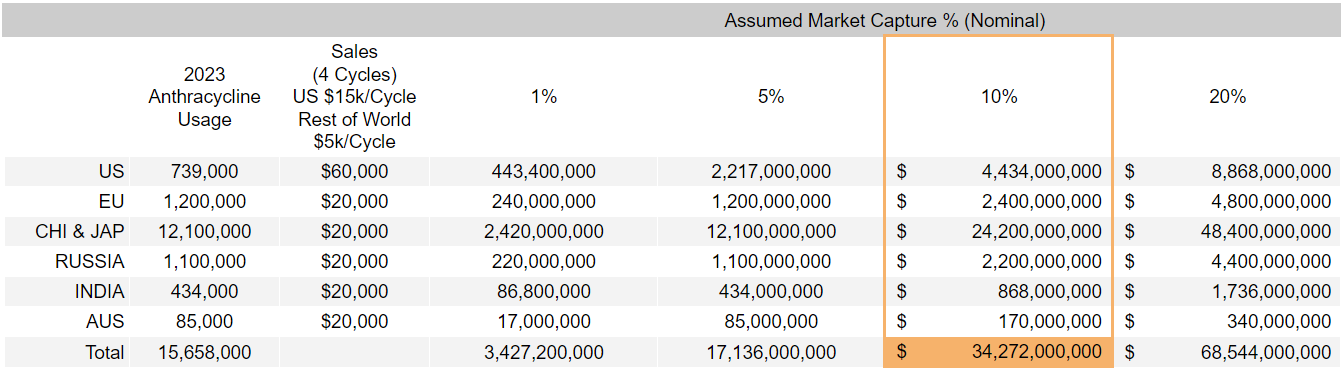
Using @johndprent data, which focuses on a single drug class, the dollar value for the Bisantrene opportunity is enormous. While necessary, estimating the global market value for Bisantrene is a difficult and dubious venture. If we assume the ~10% of cancer cell lines that demonstrate 2-fold improvement translates to patients and affords Bisantrene a 10% market capture, global yearly revenue estimates are $34.3B. This number is dumb because a 99% discounted TAM means clinical validation will sky-rocket RAC. The takeaway is the enormity of the opportunity we are invested in. Never has a drug been developed that synergistically kills cancer while providing cardioprotection - the exciting part is that each MoA appear to be universal synergistic mechanisms.
Title: Preclinical Advances of BisantrenePrice Sensitive:...





Add RAC (ASX) to my watchlist
 (20min delay) (20min delay)
|
|||||
|
Last
$1.64 |
Change
0.050(3.15%) |
Mkt cap ! $278.7M | |||
| Open | High | Low | Value | Volume |
| $1.58 | $1.65 | $1.57 | $98.54K | 60.86K |
Buyers (Bids)
| No. | Vol. | Price($) |
|---|---|---|
| 2 | 2377 | $1.59 |
Sellers (Offers)
| Price($) | Vol. | No. |
|---|---|---|
| $1.64 | 320 | 1 |
View Market Depth
| Last trade - 16.10pm 06/11/2024 (20 minute delay) ? |
| RAC (ASX) Chart |