There is no feasible production route possible without neutron irradiation.
We conclude that proposed new facilities for production of 99Mo alone will not be sufficient to maintain adequate supply of various important medical isotopes, with the highlighted example of 177Lu as an essential isotope for current and new radionuclide therapies for cancer.
To my way of thinking it would be better to place any enrichment of YB176 where it is irradiated and separated using advanced methods for separation due to it being highly radio active and it is debatable whether the OPAL reactor is suitable anyway.
Where is it possible to irradiate this YB176, I can think of one place where SILEX already has a presence?
Challenges and future options for the production of lutetium-177
Introduction
The use of the medical isotope lutetium-177 is increasing, but there are concerns that its worldwide availability may not be sufficient in the long term. This warrants an evaluation of its use and production.
Nuclear medicine involves the use of a spectrum of radioactive isotopes for diagnostic and therapeutic purposes, for example to identify cardiovascular and inflammatory diseases or to treat various types of cancer. The applied techniques require various isotopes with different physical properties. Isotopes for diagnostic purposes (gamma or positron emitters) typically decay with half-lives in the range of minutes to hours, while therapeutic isotopes (electron or alpha emitters) generally have half-lives of days to weeks. Because of this continuous loss by decay, in combination with the need to provide timely medical procedures for all patients in need, nuclear medicine requires uninterrupted and sufficient supply of relevant medical isotopes.
The applied medical isotopes have different requirements for production and distribution. For example, isotopes with longer half-lives like molybdenum-99 (99Mo) and lutetium-177 (177Lu) are typically produced by fission or activation in a nuclear reactor, and are then distributed to medical centres worldwide. Shorter lived isotopes cannot be transported over longer distances and need to be produced locally or regionally. Typical examples are technetium-99 m that is derived using a mother-daughter generator, and fluor-18 that is produced using a cyclotron. Continuous availability of all these production techniques at optimal locations is essential, in order to warrant adequate supply of every required isotopes throughout the world.
However, there is no central planning for the future of worldwide isotope production. In 2008–2010, the world started to notice this because the situation was dire: two of the main isotope-producing reactors at the time, the NRU in Canada and the HFR in the Netherlands, were both not operational unexpectedly, leading to a world-wide shortage of several medical isotopes. This caused important delays in diagnostic imaging and in treatment of cancer, and many centres struggled to find workable alternative strategies to provide adequate medical care for their patients [1]. This very challenging situation gave rise to international discussions, and efforts to improve the reliability and economic sustainability of the current production infrastructure world-wide. The OECD/NEA started the High Level Group Medical Radio-Isotopes (HLG-MR), and the EU started the European Observatory on the supply of medical radioisotopes. The situation also sparked new discussions about the future of reactor-based isotope production, and investments in nuclear production reactors are currently subject of political debate. In addition, several new alternative production methods have been proposed. Upon weighing the options for future production, it will be important to consider all relevant medical applications and their associated isotopes. However, recent discussions and proposed alternative techniques to generate isotopes are almost exclusively focussed at 99Mo [2]. Since production of different isotopes poses different technological challenges, this may lead to future situations where not all required isotopes can be produced with sufficient quantity, quality, reliability or geographic spread.
We identify 177Lu as an important example of a medical isotope that may be at risk for future shortages. The increasing demand for 177Lu is explained by its application in several current and new radionuclide therapies, most notably radiolabelled somatostatin analogs for neuroendocrine tumours and PSMA-ligands prostate cancer. In combination with the challenges related to production, this leads to concerns that the availability of 177Lu as a medical isotope may not be sufficient in the long term. In this editorial we discuss the distinctive clinical aspects of 99Mo and 177Lu, how their production routes are different, what the limitations of various available and proposed new production techniques are, and how limitations may compromise the future of various radionuclide therapies.
Lutetium-177
The medical isotope 177Lu is rapidly gaining ground as an additional workhorse in nuclear medicine. 177Lu decays to stable hafnium-177 with a half-life of 6.65 days, while emitting electrons up to 149 keV and with a maximum pathlength of 1.5 mm in tissue. 177Lu also emits photons up to 208 keV that are suitable for in-vivo biodistribution imaging using a gamma camera. Lutetium is suitable for radiolabelling of biologically active tracer molecules, with a similar chemical approach as the positron emitter gallium-68, to form a diagnostic/therapeutic pair. This allows treatment in conjunction with higher-resolution and quantitative diagnostic PET imaging for patient selection and response evaluation, a combination that is referred to as the theranostic approach [7]. These characteristics make 177Lu a very suitable isotope for image-guided radionuclide therapy [8].
The biodistribution of 177Lu was first reported in mice in 1978 [9], and this was followed by attempts to perform local radionuclide therapy with intra-articular injection in rats with arthritis [10]. After that, systemic administrations labelled to various experimental tracers were explored for multiple cancer types [11, 12]. The first mainstream application used 177Lu labelled somatostatin analogs to target well differentiated neuroendocrine tumours (NET) which usually overexpress the somatostatin receptor. This treatment is generally referred to as peptide receptor radionuclide therapy (PRRT) [13]. PRRT using 177Lu-DOTATATE is now a regular EMA/FDA-approved therapy, with proven efficacy for patients with metastatic or unresectable NETs [14]. 177Lu-DOTATATE therapy is currently also explored for several other tumour types, including for example melanoma, merkel cell carcinoma, esthesioneuroblastoma, thyroid cancer and malignant meningioma [15,16,17,18,19].
In the meantime, more biological targets have been identified that allow image-guided radionuclide therapy with 177Lu for other tumour types. Currently most promising is PSMA-directed therapy for patients with metastatic castration-resistant prostate cancer (mCRPC) who have no other effective treatment options left. In 2018 a meta-analysis of 10 studies with 455 patients receiving 177Lu-PSMA-617 therapy showed PSA response in 2/3 of patients already after one cycle, and this response was also associated with prolonged survival [20]. A recently completed multicenter phase 2 study with patients receiving up to 6 cycles Lu-PSMA at 6-week intervals (the TheraP trial), showed better PSA-response and lower toxicity as compared to cabazitaxel [21]. An international randomized phase 3 study is currently ongoing (the VISION trial), and its results are eagerly awaited [22]. A positive outcome of this study could facilitate registration of the applied 177Lu-PSMA-617, with the potential to become a new mainstream therapy for a large patient population. Other options currently under investigation include 177Lu labelled to ligands that target activated tumour-associated fibroblasts (FAPI) for various tumour types, and several other options [7, 23].
The current supply and demand situation for 177Lu is less transparent than for 99Mo. Since Lutathera currently is the only EMA/FDA-approved 177Lu-based medicine, it can be assumed that a sizable part of the 177Lu produced today is used in Lutathera. Based on the financial results published by Novartis and the list price of Lutathera, one would infer that the number of doses administered annually is around 10.000–15.000 doses of 7.4 GBq each. This is likely a strong underestimation of the total 177Lu production, if only because of significant research activity for the described new applications.
It is difficult to find an authoritative forecast of the 177Lu demand in open literature. Commercial market analysts expect a very significant growth in the demand for 177Lu in the coming years [7, 24], leading to the world demand for 177Lu multiplying several times over as a result of the introduction of new 177Lu-based medicines. The underlying reasons for this expected growth are easy to understand in global terms. The patient population that can be treated with 177Lu becomes much larger once PSMA-directed therapy becomes a regular treatment. Each year about 366.000 patients die of prostate cancer worldwide [25], of which a large part could theoretically benefit from PSMA-directed treatment with up to 6 cycles of around 7.4 GBq 177Lu. This could imply a worldwide potential for 177Lu-PSMA-ligand therapy of at least an order of magnitude more cycles (and total 177Lu dose) as compared to Lutathera. There are of course many assumptions going into this example, but it serves to illustrate the thinking behind the potentially spectacular growth that may be anticipated for 177Lu, even without considering other potential targets or patient groups that are currently under investigation.
Production of Lutetium-177
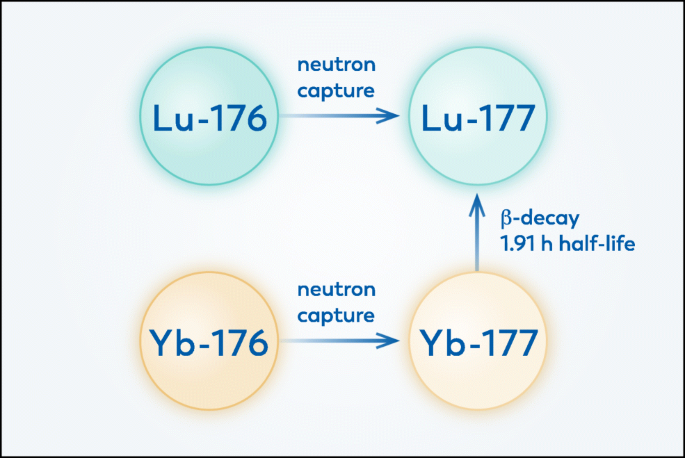
The increasing options and evidence for radionuclide therapy with 177Lu warrant an investigation of current and future production routes. 177Lu is produced in a nuclear reactor through irradiation of a source material with neutrons. There are currently two ways to produce 177Lu, the carrier added way and the no carrier added way, see Fig. 1 [26].
Illustration of possible production routes for 177Lu. Neutron irradiation of 176Lu yields carrier-added 177Lu, while neutron irradiation of 176Yb indirectly leads to no carrier added 177Lu via subsequent decay. There is no feasible production route possible without neutron irradiation.
The carrier added route uses stable lutetium as the material to irradiate with neutrons. To enhance the yield, and to prevent the creation of unwanted other radionuclides, the lutetium is enriched in 176Lu. The first advantage of this route is that the nuclear reaction occurs with high probability, so that only one milligramme of enriched lutetium is needed to produce approximately 50 patient doses. The other advantage is that the radiochemical processing after irradiation is limited to producing lutetium chloride, which is relatively simple. This route also has some drawbacks. At the end of irradiation only about 30% of the lutetium is useful radioactive 177Lu. Since the 177Lu decays while the rest of the lutetium is stable, the fraction of useful lutetium is smaller by the time it reaches the patient. The other drawback of this route is that the irradiation not only produces 177Lu but also some 177mLu, which is an unwanted beta emitter with a long half-life of 160 days that comes with additional challenges for example related to waste management.
The no carrier added route uses ytterbium as the material to irradiate with neutrons. As before, to enhance the yield, and to prevent the creation of unwanted other radionuclides, the ytterbium is enriched in 176Yb to a level above 99% [27]. The irradiation creates 177Yb, which has a half-life of under 2 h, decaying to 177Lu. One advantage of this route is that once the produced lutetium is separated from the ytterbium, the product consists of useful lutetium only with a high specific activity. The other advantage is that the decay of 176Yb to 177Lu does not co-produce the undesired 177mLu. There are however also downsides to this route. Firstly, the nuclear reaction occurs with a low probability, so that a gram of enriched ytterbium is needed to produce the same amount of activity that is reached with only a milligramme of lutetium. Secondly, the lutetium needs to be separated chemically from the ytterbium, which is a challenging process: only 1 in roughly 5000 atoms in the irradiated material is a 177Lu atom, so the chemical separation process needs to have a high separation efficiency.
For both ways of producing 177Lu, a high neutron flux is needed, albeit for different reasons. For carrier added 177Lu, a low neutron flux would lead to a low specific activity (a low ratio of useful 177Lu as a fraction of all lutetium). This can be a restriction for possible success in therapy applications. For no carrier added 177Lu, a low neutron flux poses economic and chemical challenges. The required amount of enriched ytterbium is high from the start: for the same amount of 177Lu one requires a thousand times more enriched ytterbium than enriched lutetium. If the neutron flux is significantly lower than in current-days irradiation, the only way to compensate the lower yield is by increasing the mass of ytterbium that is irradiated. But enriched ytterbium is an extremely scarce product, making it excessively expensive. Currently, the only production of enriched 176Yb comes from low-throughput facilities (calutrons) in Russia [28], which is a problem anyway for the future of carrier-free 177Lu production. Lower neutron fluxes would not only aggravate this problem, but also increase the chemistry challenge: the reduced number of 177Lu atoms in the matrix of ytterbium below 1:5000 would require a separation efficiency that has, as yet, not been achieved.
It is not feasible to produce 177Lu by nuclear reactions that are initiated by something other than a neutron. There is no useful target that can be irradiated with an accelerated proton, or any other particle, to produce 177Lu. The only stable nuclides close to 177Lu on the nuclide chart apart from 176Yb and 176Lu are hafnium isotopes (e.g., 178Hf). Even the most promising nuclear reactions that would produce 177Lu via such routes are at least 50 times more unfavourable [29] than the reaction currently employed for no carrier added 177Lu, which itself is not very favourable. In addition, irradiation volumes in accelerators inherently need to be small. Therefore, accelerators cannot offer a viable alternative for large-scale 177Lu production. Types of production facilities
It follows that a high neutron flux is highly desirable, if not mandatory, for 177Lu production. Current production of 177Lu, both for carrier added and no carrier added 177Lu, is done in reactors with a high neutron flux (in alphabetical order): BR2 (Belgium), FRM-II (Germany), HFR (Netherlands), IVV-2 M (Russia), LVR-15 (Czech Republic), Maria (Poland), MURR (USA), OPAL (Australia), Safari (South Africa), and SM-3 (Russia). These facilities have been designed specifically to generate high neutron fluxes. Except for FRM-II and OPAL, these reactors are more than 40 years old. The question is whether new facilities with a low neutron flux, that have been designed almost exclusively for 99Mo production, can be competitive for 177Lu production. The answer to this question can be given by dividing the various proposed facilities in four categories.
Power reactors
Bruce Power, Framatome and Kinectrics have a collaboration to start 177Lu production based on irradiations in Bruce Power reactors [31]. Contrary to all other reactors used for isotope production, these reactors are part of a nuclear power plant. The reactors are of the CANDU-type that allows on-line loading and unloading, which is necessary for producing isotopes with a half-life that is much shorter than the cycle length of a power plant. It is not immediately clear at which flux these irradiations take place, but it stands to reason to assume that the flux is high enough for a decent 177Lu yield. Also, the amount of space available in large reactors like these can be expected to be more than sufficient for this purpose. These reactors can be competitive for 177Lu production, provided one is willing to use the reactor space for this purpose, and willing to allow frequent loading and unloading of isotopes in a power station.
The catch with this initiative is that the isotope production clearly takes a back seat to electricity production. The latter brings in far more income, and when this becomes uneconomical for whatever reason, the isotope production will go down with it. In addition, it is important to note that the CANDU reactor type is the only one in which isotopes can be loaded/unloaded during operation, that only 7% of the power reactors is of this type, and that currently there is no CANDU reactor planned to be built or under construction. The newest CANDU reactor at the Bruce Power site in Canada started operations in 1987. In Europe there are only 2 operational CANDU reactors, both in Romania. It is questionable whether future isotope production should be dependent on the success and availability of CANDU reactors in the world of electricity production. Conventional ‘research’ reactors
There are a number of initiatives to build new reactors of the ‘research’ type. Perhaps a more appropriate name is ‘multi-purpose’ reactors, because often they can be used for isotope irradiations as well as for test irradiations of nuclear materials and fuels. For some of these initiatives, isotope production is one of the stated design goals, and in these cases a high flux is generally part of that design goal. As a result, these reactors will have a high neutron flux allowing them to be competitive for 177Lu production. Examples are KJRR (Korea), Pallas (Netherlands), and RA-10 (Argentina). One can also consider a number of initiatives for new reactors that may not have isotope production as their primary goal, but that could contribute to isotope production at some point in the future. Reactors such as JHR (France) and MYRRHA (Belgium) can be expected to be competitive for 177Lu production, at least if they will be engaged for this purpose.
A downside to the construction of new specifically designed reactors is the cost of development, that needs to generate a return on investment mainly through commercialization of the produced isotopes. This requires a long-term business case with regard to medical isotopes for diagnostic and therapeutic purposes. Discussion
In the coming years, production of medical isotopes will remain a matter of clinical, financial and political debate. There are multiple routes to production of 99Mo, potentially involving investments in several current and new techniques. But it remains a vital question whether future facilities, of which an increasing number may be optimized for 99Mo production alone, can also produce the full range of other required medical isotopes.
We identify 177Lu, which already is an indispensable isotope for radionuclide therapy and will become even more so with increasing number of treatable prostate cancer patients, as an important candidate isotope that may not be produced in sufficient quantities in the near future, in case of insufficient availability of high-flux neutron irradiation facilities. In 2015, Dash et al. provided a prior technical overview of production routes for 177Lu [26]. Since that time, new options for production routes were proposed and developed for 99Mo but not for 177Lu. We explained how the production of these isotopes is different, and why the production of 177Lu will require continued availability of high-flux neutron irradiation facilities.
There are many other nuclides with a potentially bright future in nuclear medicine, comparable to 177Lu, that have not been given sufficient attention even though they pose different requirements on the production technology. Examples of other therapeutic isotopes for which reactors with high neutron flux are essential include (but are not limited to) yttrium-90, samarium-153, iridium-192, tin-117 m, and lead-212. The reactors that produce 177Lu today are well equipped to produce these isotopes as well, but alternative technologies proposed for 99Mo production are ill suited for this purpose. As a result, the future of a broad range of isotopes depends on nuclear reactors of the conventional type.
The long-term supply of medical isotopes is becoming an urgent issue. While the isotope demand is set to increase over the coming years, current reactor facilities are generally quite old and their reliability for uninterrupted production will reduce over time. The construction of a new reactor facility requires political approval, funding, design, construction, and validation, a process that typically takes about 10 years in total. Political awareness of this challenge is crucial to ensure continued supply of all required medical isotopes. To achieve this, the ongoing debate about the relevance of nuclear production reactors needs to be supported by representatives of the medical field who have knowledge of the various production techniques and their limitations. Conclusions
We conclude that proposed new facilities for production of 99Mo alone will not be sufficient to maintain adequate supply of various important medical isotopes, with the highlighted example of 177Lu as an essential isotope for current and new radionuclide therapies for cancer. Continued investments in high-flux neutron irradiation facilities will be crucial to maintain sufficient availability of lutetium-177 and other medical isotopes, in order to provide required both diagnostic and therapeutic medical care for many patients in the coming years.
A personalised tool to help users track selected stocks. Delivering real-time notifications on price updates, announcements, and performance stats on each to help make informed investment decisions.





 (20min delay)
(20min delay)