
ULCERATIVE COLITIS
A new chapter ….
Amy Lightner’s poster abstract 407B was presented at the worlds largest annual IBD conference ECCO2022 last weekend. It is easy to overlook an the interim analysis of a Phase 1/2a for the first recruited 6 patients (4 treated/2 placebo) with moderate medically refractory Ulcerative Colitis….but if the rest of the patients in this trial have similar outcomes , big Pharmas tongues should start to wag …and maybe faces at the FDA should start to go crimson/scarlet. They certainly should after their pointless CRL for Ryoncil when all that was needed was a conditional approval with a confirmatory trial …as evidenced by their own FDA ODAC panel of experts agreeing 9-1 that our therapy for an unmet need (under 12 )should be available for use .
P407 A Phase IB/IIA study of remestemcel-L, an allogeneic bone marrow derived mesenchymal stem cell product, for the treatment of medically refractory ulcerative colitis: An interim analysis
Lightner, A.(1);Dadgar, N.(2);Fulmer, C.(3);Ream, J.(4);Nachand, D.(4);Steele, S.(2);
(1)Cleveland Clinic, Department of Colorectal Surgery, Cleveland, United States;(2)Cleveland Clinic, Colorectal Surgery, Cleveland, United States;(3)Cleveland Clinic, Pathology, Cleveland, United States;(4)Cleveland Clinic, Radiology, Cleveland, United States;
“In the treatment group (n=4), the Mayo score and Mayo endoscopic severity score decreased in all patients by two weeks after MSC delivery. By six weeks post MSC treatment, all treated patients had achieved clinical and endoscopic remission as defined by the Mayo score and Mayo endoscopic severity score………..
In the control group (n=2), the Mayo score did not decrease. Patient reported number of daily bowel movements increased as did the number reporting blood in their stool; urgency remained unchanged. With regard to patient reported outcomes, at three months, based on the IBD-PRTI, one patient was neutral, and one patient was dissatisfied. Treated response was described as poor…”
In relation to these trial results , remember the previous Mesoblast ASX disclosure written below in full , from Fred Grossman about the overlapping pathophysiology between sr aGVHD and UC/Crohns Disease (CD) (see link below). The latter two are so close in profile that a considerable number of patients remain unclassified between CD/UC…particularly in young children.
“NEW YORK, Oct. 22, 2020 (GLOBE NEWSWIRE) -- Mesoblast Limited (Nasdaq:MESO; ASX:MSB), global leader in allogeneic cellular medicines for inflammatory diseases, today announced that a randomized, controlled study of remestemcel-L delivered by an endoscope directly to the areas of inflammation and tissue injury in up to 48 patients with medically refractory Crohn’s disease and ulcerative colitis has commenced at Cleveland Clinic.
Mesoblast Chief Medical Officer Dr Fred Grossman said: “Inflammation of the gut in Crohn’s disease and ulcerative colitis closely resembles the most severe manifestation of advanced-stage, life-threatening acute graft versus host disease (aGVHD). Mesoblast’s objective is to confirm the potential for remestemcel-L to induce luminal healing and early remission in a wider spectrum of diseases with severe inflammation of the gut, in addition to steroid-refractory aGVHD.”
Mesenchymal stem cells (MSCs) promote healing of inflamed gut tissue by downregulating gut mucosal effector T-cell activity and promoting regulatory T-cell formation. MSCs have been tested in clinical trials of Crohn’s disease using two different modalities: intravenous infusions of MSCs to treat the primary inflammation of Crohn’s disease and local injections of MSCs to treat fistulae complicating Crohn’s disease.
A third modality, endoscopic delivery of MSCs, has been successful in preclinical experimental models of colitis, reducing the excessive cytokine storm in the inflamed gut and resulting in tissue healing. The study at Cleveland Clinic will be the first in humans using local delivery of MSCs in the gut, and will enable Mesoblast to compare clinical outcomes using this delivery method with results from an ongoing randomized, placebo-controlled trial in patients with biologic-refractory Crohn’s disease where remestemcel-L was administered intravenously.
The study’s lead investigator Dr Amy L. Lightner, Associate Professor of Surgery in the Department of Colon and Rectal Surgery at Cleveland Clinic, stated: “We are aiming to establish a new treatment paradigm by administering remestemcel-L at one of two escalating doses, or placebo, directly to inflamed gut tissue in patients with medically refractory Crohn’s disease and ulcerative colitis, both highly debilitating conditions with significant, unmet medical needs.”
According to recent estimates, more than three million people (1.3%) in the US alone have inflammatory bowel disease, with more than 33,000 new cases of Crohn’s disease and 38,000 new cases of ulcerative colitis diagnosed every year. Despite recent advances, approximately 30% of patients are primarily unresponsive to anti-TNFα agents and even among responders, up to 10% will lose their response to the drug every year. Up to 80% of patients with medically-refractory Crohn’s disease eventually require surgical treatment of their disease, which can have a devastating impact on quality of life.”
———————————————————————————————————————————————
So despite the tiny sample size of this initial cohort in the ECCO2022 published poster .. and I suspect, moderate severity of the treated patients (in keeping with the safety objective of a Phase 1/2a trial) …What can we determine? Firstly , the blindingly obvious , how could the results show a better outcome than 100% remission !!!
To achieve clinical and endoscopic remission in the first 6 weeks,whilst the control fails to show any improvement of deteriorates is exemplary. If the rest of the 6 cohorts out of 24? achieves even 60% remission at six weeks we will have a very valuable potential therapy…WITH NO ATTRIBUTABLE SIDE EFFECTS. The trial protocol also affords patients on placebo with the opportunity after 3 months, to cross over from the control to MSC therapy . Can you imagine how achieving remission with any of those placebo patients will look? Talking of These randomised results target many of the same inflammatory signalling pathways (particularly TNF Alpha) as for steroid refractory aGVHD …which further confirms the activity of our cells in the gut …and continues to add to the amazing safety profile of mesenchymal cells, now validated by over 50,000 patients in worldwide clinical trials to date .
In theory, IF, Remestemcel has the same affect on Crohn’s Colitis and can heal the mucosal lining so efficiently as to put patients into “deep remission”, then there might be little need to treat the longer term symptoms of complex perianal fistulas… which occur in approx 1 in 4 patients. I have had not had time to fully consider the interim analysis results from the CD trial also being conducted at the Cleveland Clinic by Amy Lightner …Poster P428, which treated 6 Crohns Colitis patients with Remestemcel ..but I would suggest people ignore the subjective CDAI scoring (a composite score which is largely discredited) and look at the primary measure of CD activity, which is faecal calprotectin (F/Cal) in the stool. In combination with SES-CD scores there is a lot of positive healing activity shown in the first four treated patients.
Takeda have spent the best part of a US $1 billion on the fistula opportunity(Alofisel)…having purchased TiGenix for $608m in 2018…and are now paying for a Phase 3 trial in the US. What a bummer ! (Sic Ed)
The standard treatment for milder UC (and CD) is often mesalamine (5 ASA) whose precise mechanism was of course unknown when it was approved in the US . It is marketed under various brand names, including Pentasa (Takeda). If normal first line therapies fail then corticosteroids are normally taken. Whilst very cheap mediators they obviously have potent side effects, especially in relation to their immunosuppressive properties leaving patients highly vulnerable to infection . If the patient becomes refractory …then TNF inhibitors such as Infliximab / Janssen Bio/J&J) are often the gold standard. Brand names Remicade/Inflectra/Renflexis… but now with numerous bio similar competitors . MOA TNF …showed in its landmark ACT2 trial, a remission rate of 30% (13% placebo)….with cost understandably having a major influence on first line therapies chosen . So, i thought it might also be helpful to list some of the remission rates shown by some of the most used alternatives for UC to put our results in context … particularly for patients who are medically refractory (mainly anti TNFs), which is the inclusion criteria for enrolment . The problem with quoting these rates is they are sometimes flattered by inclusion of some biologically naive patients , (as opposed to refractory)who often have superior remission compared with baseline characteristics . Much of the data shown below was sourced from an article linked below from the BMJ published in April 2021showing consensus agreement on real world treatments by specialist practioners.
https://gut.bmj.com/content/68/Suppl_3/s1
So, how does Remestemcel-L’s clinical and endoscopic remission rates of 100% compare to its peers that used alternative MOAs at the same 6-8 weeks timescale in analysis of moderate to severe UC ? Please remember this is an interim analysis of a Phase 1/2a representing an initial 6 out of 24 treated medically refractory patients for UC , randomised 2 for 1 with placebo. I should also point out again that these first 6 patients appear to have been quite mild cases at baseline , but we are talking about chronic long term UC sufferers… who look as though they have exhausted most other treatment options and may potentially need surgical removal of the large bowel if no other therapeutic options are available. Many of the patients treated will relapse, even with the anti TNFs treatments. For example, a significant number of patients achieving clinical remission at 12 months taking Stelara had to intensify their dose to remain in remission …suggesting less favourable outcomes for some over a longer period …and Stelara has some of the best in class non relapse results.
https://clinicaltrials.gov/ct2/show/NCT04543994
UC eligibility requirements for Remestemcel -L trial at Cleveland Clinic
The following medications/therapies must have been discontinued before first administration of study agent:
- TNF-antagonist therapy (eg, infliximab, etanercept, certolizumab, adalimumab, golimumab), vedolizumab, ustekinumab for at least 4 weeks.
COMPETITOR BENCHMARKS.
Most of the competitor comparatives in the medically refractory (mainly Anti TNF) class, are taken directly from the BMJ article, are summarised below, combined with their 6/8 week clinical remission rates where easily available . Please remember that many of these therapies achieve higher 12 week remission rates or have maintenance studies or 1 year remission showing much superior findings. Typically a significant part of population studies have patients relapsing over the course of a 12 month treatment..so you need to research individual trials to get a full sense of comparability.
Tofacitinib/ Brand Name Xeljanz MOA JAK inhibitor (No2 treatment in Europe) after Infliximab. In the OCTAVE 1 trial of 589 patients was reported to achieve a clinical remission of 11.4%. As an orally administered therapy it is preferred by some practioners.
(In the JAK class , the much fancied (not by me) Filgotinib/ Brand name Jyseleca, developed by the Belgian/ Dutch biotech Galapagos NV , has just received EMA approval but has very little prospect of FDA approval having recently been dropped by Gilead .)
Adalimumab/AbbVie Brand Name Humira (the worlds best selling drug ..recently the subject of massive price discounting from bio similars).AbbVie are now introducing Skyrizi and Rinvoq as patented alternatives. Humira achieved 21% clinical remission at weeks at in the Ultra 1 trial .
Vedolizumab / Takeda Brand Name Entyvio, MOA Integrin binder. The treatment produced a very interesting trial protocol in its 895 patient GEMINI trial , which makes straightforward comparisons concerning clinical remission rates rather tricky. Performed better in The VARSITY trial comparing Vedolizumab with Adalimumab… but real world data is reported to suggest that it is equal with Infliximab in treatment naive patients.
Golimumab/ TNF inhibitor. Brand Name Simponi…Janssen Bio US and Schering Plough/Merck (Europe) and Mitsubishi (Far East). In 1064 patient PURSUIT trial achieved a clinical remission rate of 17.9% at week 6
Ustekimumab/ J&J Brand Name Stelara MOA IL12/IL23 blocker.. has recently received FDA approval for UC . reported to have achieved a 15.6% clinical remission rate in the UNITI trial at 8 weeks.
Deucravacitinib / Zeposia MOA TYK2 inhibitor . Bristol Myers Squibb In Oct 21 , failed to meet primary endpoint in P2 UC trial .
Assoc. Prof Amy Lightner at the Cleveland, who is conducting this trial , is one of the foremost authorities on the practical use of mesenchymal cells in Crohn’s disease. In addition to her consultancy work with Takeda regarding EMA approved Alofisel (using adipose tissue for peri anal fistula which she has also played a substantive role in a trial using autologous MSCs sponsored by the Mayo Clinic whose “ Mayo scores” are used a gold standard for clinical evaluation . She is also currently conducting a cross over trial with 40 patients and is examining MSC treatments for rectovaginal fistula which occurs in 10% of female Crohns patients.
Remestemcel might prove particularly helpful for paediatric UC sufferers who often have a particularly poor prognosis as they have much higher colorectal cancer rates in addition to often complex cases.
Dr Bauer, at OTAT, LOOK AT THE ADVERSE EVENTS OF THE ALTERNATIVE TREATMENTS. You employer has approved JAK inhibitors like Tofacitinib and Ruxolitinib with black box warnings…then bolted the stable door on our perfectly safe treatment like Remestemcel on the pretext of potency assays when clinical results closely match our longstanding EAP results and the excellent record of Temcell in Japan . You moan about wanting two RCT’s for sr aGVHD trials which is a small population with an unmet need. Were you consistent with other GVHD therapies you approved , such as open label Phase 2 for Kadmon Pharma (belumosudil) , or Novartis (Rux) or AbbVie (Imbruvica)….who gained approval using single non randomised Phase 3 trials .Now your organisation looks pretty stupid in relation to a whole asset class of inhibitor therapies …which some might say you have shown preferential treatment to. It’s a bit late now.
To the parents of children over 12 , with steroid refractory acute GVHD, you should be asking how the FDA has approved a therapy, which, independent of the toxic side effects has very poor efficacy in the most severe classes of patients. Equally the “forest tree plots” for higher grade liver, upper and lower GI or multi organ look very disappointing relative to some other treatments such as ECP or MSCs. Look at the links for the Reach 1 & Reach Phase 2 trials for Ruxolitinib and check for yourself the efficacy rates achieved in the higher grade patients. Let me give you a taster. In Reach 1 ,the 15 patients for Ruxolitinib showed an average of 26.7% for all liver grades above O ! Although 56 patients with a very lowest liver grade had somehow been included with a reported ORs of 62.5%. This compared to 62% in “any liver” in Mesoblasts EAP. Remember in Protocol GVHD001 89% of Mesoblasts patients had Grade C/D at baseline compared to 67.6% (48/71) in Reach 1….Mesoblast had 49% enrol with Grade D in GVHD001 compared to less than 20% (14/71) in Reach 1….and the FDA lecture us about null hypothesis rates while Incyte/ Novartis used their trial investigator to chose which best available therapies to compete against. Unsurprisingly, despite the high success rate of MSCs , when used for a small number of patients in one of the Reach trials, they never seem to end up in a head to head trial against us….for obvious reasons.
https://www.nejm.org/doi/pdf/10.1056/NEJMoa1917635. Reach2
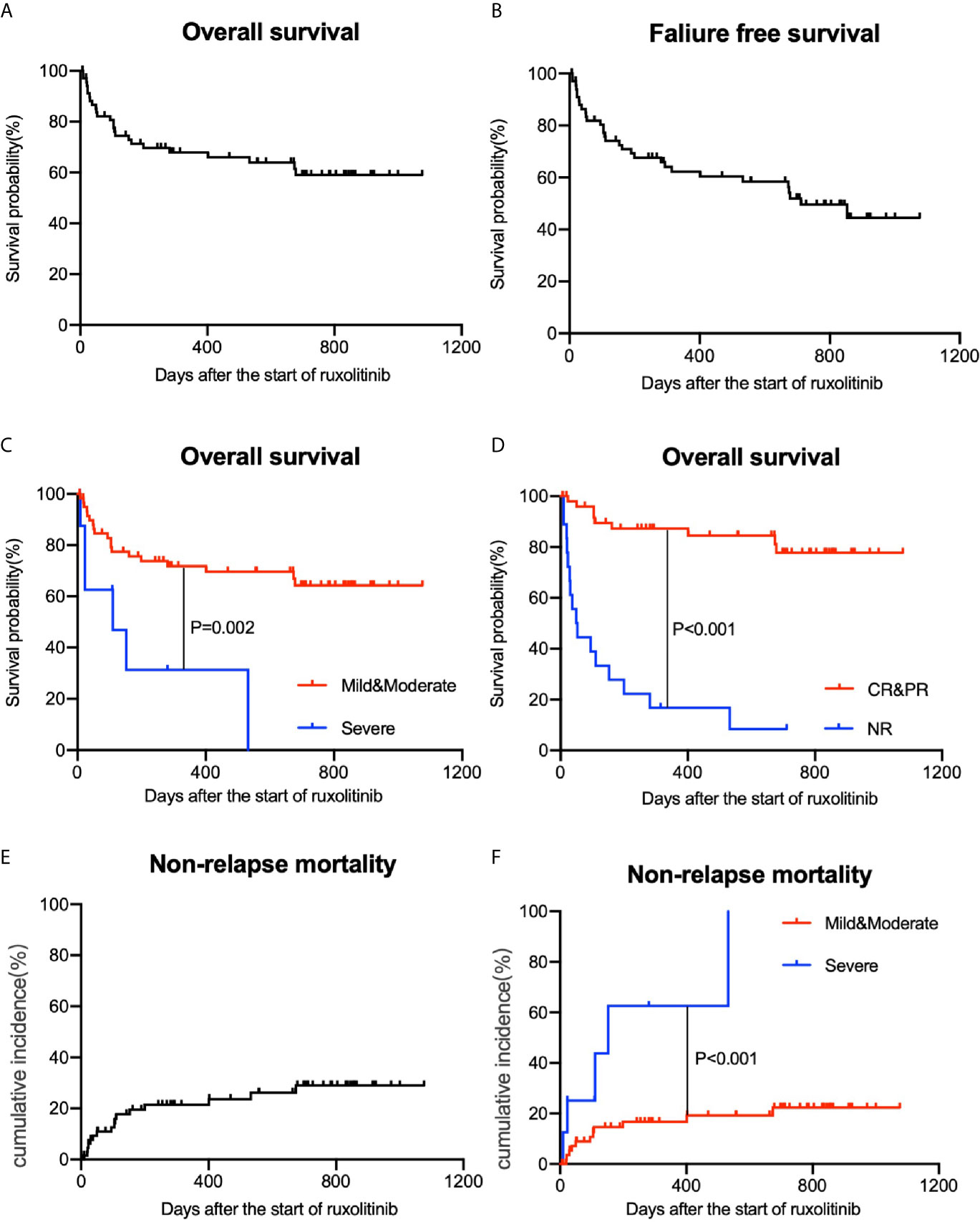
When Ruxolitinib was used as a salvage therapy in chronic GVHD , (graphical illustration below of non relapse mortality and overall survival) the study was published in Frontiers and the outcomes of the non responders gives you a good idea what I am talking about .
It’s just not acceptable that a treatment with such low rates of efficacy in non responders ,is the only treatment allowable for adult sr aGVHD … The FDA wants to delay the advancement of perfectly safe Mesenchymal cell therapies (which are twice as effective in many non skin categories) , while they try to perfect protocols for cell characterisation and improve on of our in vitro potency assays (TNFR1 and IL2R ) to show in vivo activity .... Maybe they should be asking why we have such superior results to Ruxolitinib in the sickest graded patients… backed up by retrospective analysis of patient data for ST2/Reg3a , the most accurate bio marker scores for sr aGVHD.
Steve Bauer at OTAT , who seems to be calling the shots while Peter Marks, his boss, smiles supportively at everyone in the background…..Bauer is a career man at the FDA and I am sure his intentions and those of his team , are both logical ,honourable and sincere…but that ODAC document embarrasses the both the impartiality and high standards expected of the FDA. (I will cover this separately, but basically they either used combination therapies or studies with very poor durability of effect to question the null hypothesis for OR at 28 days ) .OTAT has built it own little empire and rather than just review studies it is busy trying to create its own…with pitiful budgets compared to the serious players in this space. Luckily their own FDA experts on the ODAC panel ignored their opinion (which I believe was arrived at using a flawed comparability study of the null hypothesis) and still recommended the use of Remestemcel. That is not to say that Mesoblast is perfect…Prof Itescu acknowledged that they did not have sufficient comparability data over a wider population of patients to be able to utilise some more recent relevant potency assays, particularly in relation to T cells and TREGS…nor will it be possible to know the exact mechanism of action in such a multi factorial immune pathway therapy …Bauer is right about the need for the right CQA’s but as many experts opined on the ODAC panel, many of these questions will not be answered even if Meosblast came back with the results of a further RCT P3.
So Peter Marks. Look at the safety and efficacy profile of Remestemcel and stop prevaricating.
I think in my next article i might start to detail complete some of the outrageous shortcomings in the review document provided to the ODAC Committee by the FDA, particularly in relation to the examples used in the null hypothesis slides. In other areas, such as morphology , you would think that they discovered passage population number doubling cytoskeleton morphology when Kaplan was writing papers about it back in 2000’s. Just being well intentioned does not hack it with me. If any Americans are reading this article …just do a price check on Pentasa (first line treatment for mild UC and Crohns) in Europe and in the USA …and ask what is the FDA and the US Government really achieving ?
After all , someone has to pay for all this dithering and grandstanding…hopefully its just Dollars and not the unnecessary death of a loved one unable to get a proper treatment in time.
As to the wonderful intentions of the short sellers/non holders who are so keen to ignore the superb clinical data, to warn us shareholders about potential class actions …we know about the extreme depths some of you will go to spread misinformation and despair. May you rot in hell for all the innocent lives you destroy at the same time.
I know most of you are waiting for a liquidity event at Mesobladt such as a dilutive equity raise to close your positions..well I think you might well be disappointed…just like you were after the Grunenthal, Tasly , and Oaktree deals. The latter represented a material upgrade in terms of capital repayment timelines relative to the Hercules facility it replaced …Silviu should now have time to leverage off his IP estate, particularly in back and heart, to give you all very sore bottoms …i just wish it was several peri anal fistulas each for the lot of you ! By the way don’t forget that as soon as Kadmon cleared FDA approval for cGVHD it was snapped up for $1.6 bn by Sanofi. ….with just one advanced indication ….and Mesoblast has three/five blockbuster indications. Insane valuation…in my opinion OP
https://www.sanofi.com/en/media-room/press-releases/2021/2021-09-08-07-00-00-2293017
General Disclaimer.
Please do not rely on any of the opinions or facts represented in the above article, which may contain material inaccuracies, when making an investment decision. I am writing this article to help people make informed decisions and because there is so little up to date research available . I own the shares . I am not a medically qualified individual. Without a regulatory body like the FDA, I do accept there would be abject chaos and people would not trust the safety and efficacy of medications. The FDA has made a Herculean effort to approve vaccines that have kept most of us safe from the Covid pandemic and we should all be extremely grateful for their endeavours in this regard.
The FDA regularly issue CRLs to many other companies. I do accept that a CRL is not necessarily a “NO”decision…but often a “Not Yet” one…….but paediatric sr aGVHD is an unmet need as well as an orphan indication. Stop trying to cover your backsides. It’s safe and it works great after real world data from almost 1000 patients….AND IT DOES NOT HAVE HARMFUL SIDE EFFECTS LIKE THE ONE YOU APPROVED for children over 12 . I rate the opinion of Prof E Levine at Mount Sinai Acute International Consortium (MAGIC) and Prof Joanne Kurtzberg of Duke University and the view of your own expert ODAC panel over all your specialist team combined . It’s taken you the best part of ten years to get this right..but I guess its a bit like turkeys voting for Christmas since you all are pursuing your own research agendas which are normally years behind cutting edge science . Now with the latest evidence on glycosis influenced apoptosis ..I suppose you will want to start all over again.
That does not excuse why this regulatory organisation continues to be so slow to approve Mesenchymal cell therapies which are widely available and working perfectly safely in many other jurisdictions like Japan (Temcell/Alofisel ) Korea and Europe (Alofisel) …whilst allowing less efficacious alternatives to be prescribed in their place. You should all be disgusted .
ULCERATIVE COLITISA new chapter …. Amy Lightner’s poster...





{kind=link}
Add MSB (ASX) to my watchlist
 (20min delay) (20min delay)
|
|||||
|
Last
$1.38 |
Change
-0.080(5.50%) |
Mkt cap ! $1.569B | |||
| Open | High | Low | Value | Volume |
| $1.43 | $1.43 | $1.37 | $5.321M | 3.829M |
Buyers (Bids)
| No. | Vol. | Price($) |
|---|---|---|
| 4 | 12214 | $1.38 |
Sellers (Offers)
| Price($) | Vol. | No. |
|---|---|---|
| $1.38 | 37660 | 5 |
View Market Depth
| Last trade - 16.10pm 16/10/2024 (20 minute delay) ? |
| MSB (ASX) Chart |