This is a subject which I have a great interest in.
Therefore, perhaps others may find this interesting and could add to this. Thank you.
What They Don’t Tell Us About Treating Pain
Exposing the pain industry and the forgotten treatments for pain
READ IN APP Story At Glance
Spinal pain affects millionsdespite over $134 billion spent annually in the USA alone, with most patients remaining stuck in chronic pain cycles due to treatments that address symptoms rather than root causes.
Common pain generators are frequently missed, including tight muscles, structural misalignments, trapped emotions, and inflammatory conditions—leaving patients to cycle through increasingly dangerous interventions without addressing underlying issues.
Conventional medications create more problems than they solve: NSAIDs are the leading cause of drug-related hospital admissions, Tylenol causes 56,000 ER visits annually from toxicity, and **apentin provides minimal benefit while causing cognitive effects such as drowsiness.
Corticosteroids, despite being "wonder drugs," cause devastating long-term damage,including 5-15% yearly bone loss, 70% weight gain rates, and dramatic increases in heart attacks (226%), heart failure (272%), and strokes (73%).
Spinal surgeries remain highly profitable but questionable in effectiveness, with significant risks that patients often don't learn about until after complications occur, and no ability to "undo" surgical damage.
DMSO offers a paradigm shift: providing pain relief comparable to opioids through safer mechanisms, actually healing underlying conditions, and showing remarkable results even in severe cases like paralysis—with decades of research and thousands of testimonials supporting its safety and effectiveness.
Most patients with chronic pain will typically first be recommended a variety of pain medications and physical therapy, then once those fail, steroid injections, and then a joint surgery. Unfortunately, each step in this process is often ineffective at addressing the patient’s pain or creates a variety of complications that make their situation even more unbearable. For this reason, it is critical to understand the risks of each part of this process and the safer alternatives that can permanently alleviate joint and spinal pain.
Note: persistent or recurrent pain after spinal surgery, back pain following spinal surgery is referred to as “Failed Back Surgery Syndrome” and affects between10-40% of people who receive a spinal surgery.
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber. To see how others have benefitted from this newsletter,click here!
Common Spinal Pain Generators:
In most cases, joint pain has a cause that must be identified to treat it. For example, when treating spinal pain, we find it is critical to address:
Tight muscles—rarely recognized despite being common (particularly of the iliopsoas and quadratus lumborum—two large and frequently tight muscle groups which directly attach to the lumbar spine). Physical therapists typically focus on strengthening rather than stretching/releasing tight muscles.
Misalignment—requires adjustment and lifestyle corrections. A common cause of misalignment are uneven leg lengths which tilt the pelvis and hence the spine (and can be corrected with an appropriate heel lift).
Ligamentous laxity—often the primary cause of spinal arthritis, muscle tightness, and disc problems as tight ligaments are necessary to ensure bones stay in the correct location and do not impinge tissues.
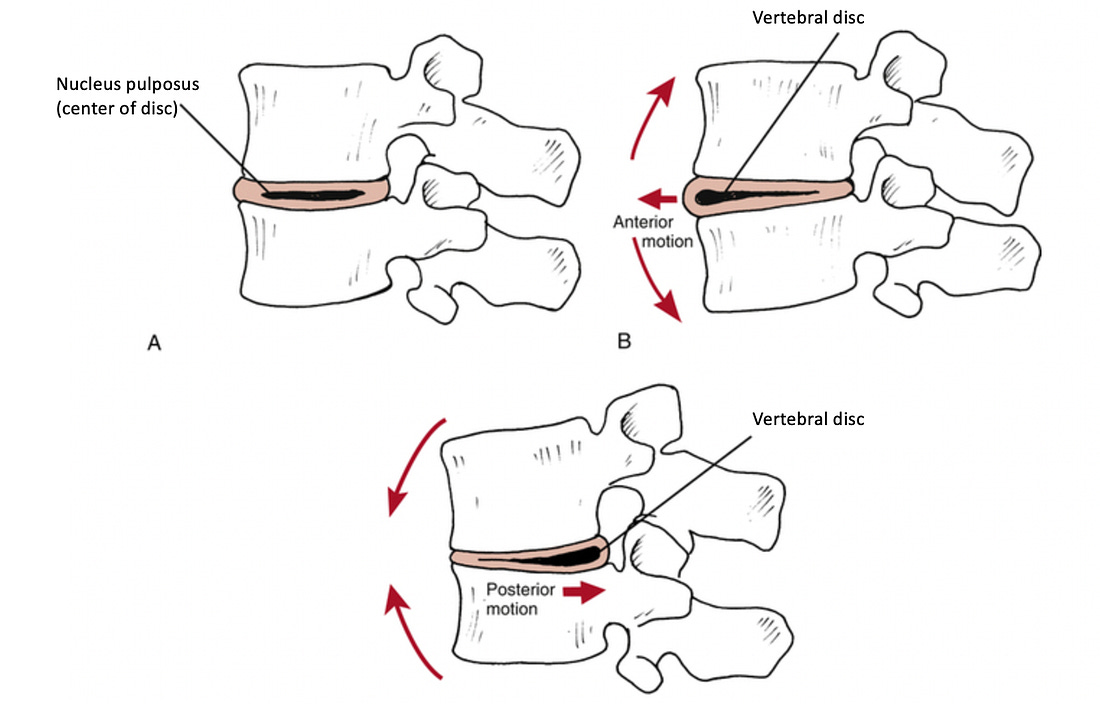
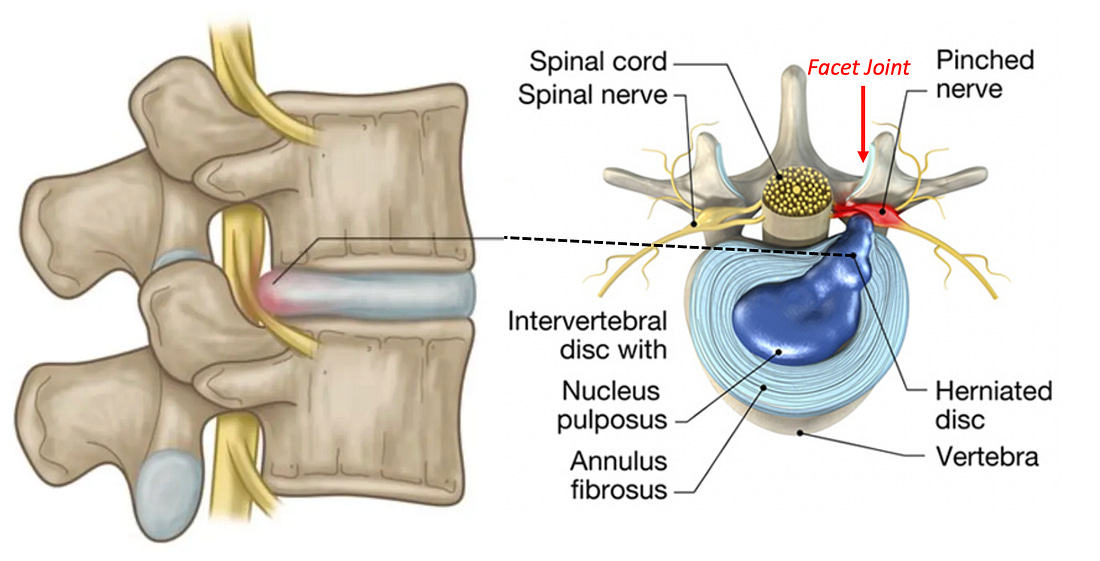
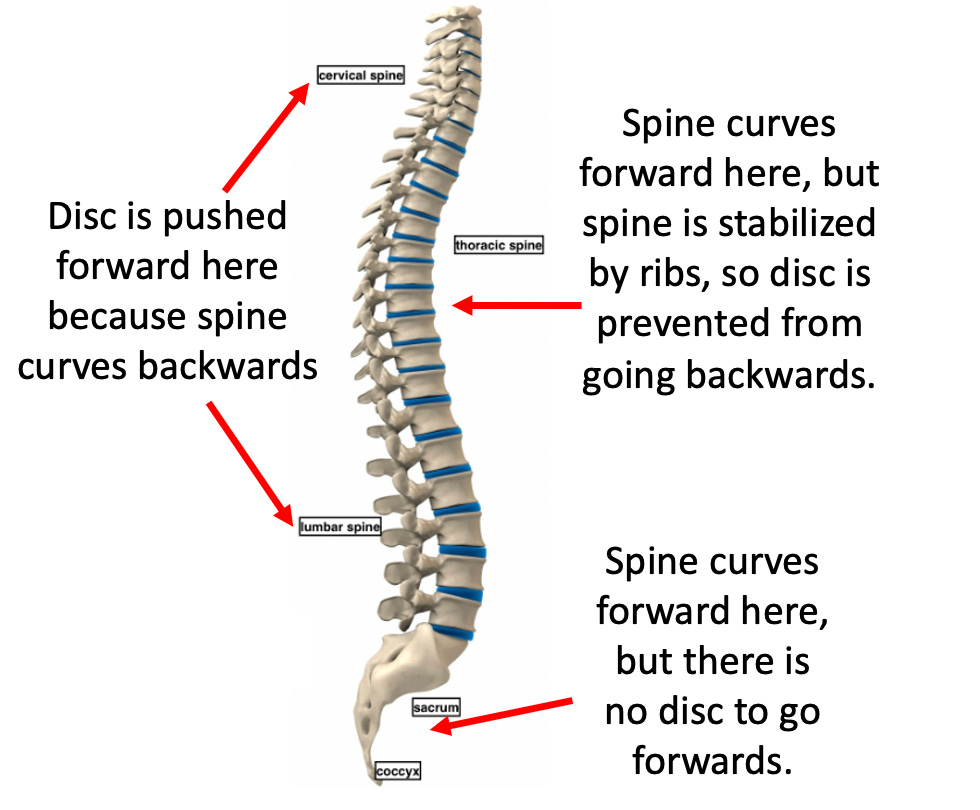
Disc herniation—not the most common cause of back pain but sometimes a significant contributor (and frequently used as a justificationfor disastrous spinal surgeries). In most cases, disc herniations result from vertebrae bending too far forward, which pushes the discs back and compresses the nerves behind them.
This can frequently result from a weakening of the spinal ligaments or poor posture which eliminates the natural backwards curve in the neck and low back.
Note: tight muscles, joint misalignments, and ligamentous laxity also create issues in other regions of the body (e.g., the knees).
Additional Pain Generators:
Trapped emotions:chronic stress and emotional distress frequently exacerbate pain (and in some cases are the primary cause of back pain). Dr. Sarno for example, addressed back pain through psychotherapy andgenerated a large followingas his approach helped many (but not everyone).
Note: we frequently finda direct release of trapped emotions(rather than psychotherapy) is necessary to address chronic emotional trauma.Nervous system dysregulation—over-activation of the sympathetic nervous system alongside under-activation of the parasympathetic system exacerbates pain.
Note:A common effect of unresolved traumais fight-or-flight system over-activation.Chronic inflammatory conditions(e.g., dietary allergies, mold toxicity, Lyme disease, spike protein injuries) often worsen pain patterns.
Note: many individuals have found thateliminating dietary food allergens resolves arthritis.Scarsfrom surgeriescan frequently generate significant autonomic dysregulationand pain, and frequently, treatment of those scars yields dramatic improvements.
Altered brain pain processing—often due to chronically over-activated nerves ormicrostroke injuring the thalamus(which otherwise dampens pain signals). In these instances, small stimuli can be extremely painful.
Systemic Medications
Since joint or spinal pain has multiple causes and diagnosis is time-consuming, physicians typically prescribe pills or refer patients elsewhere rather than address the root causes of their pain. Common medications include NSAIDs, Tylenol, Steroids, **apentin (or Lyrica), and Opioids—all with major issues.
Note: due to the high rate of addiction which follows opioid prescriptions (and the societal damage that follows), more and more, the government has moved to restrict opioid prescriptions. Because of this, patients in significant pain who will only respond to opioids, despite their best efforts, often cannot get these drugs and instead are given another ineffective option (e.g., NSAIDs), hence making it imperative that effective non-opioid solutions for pain be made available to the public.
NSAIDs
NSAIDs (e.g., ibuprofen, naproxen) temporarily reduce pain but only partially, leading patients to overuse them—often dangerously, as NSAIDs are toxic at high doses (which frequently occur since NSAIDs are taken for pain and are available over the counter). Many consider NSAIDs among the most hazardous drugs in the U.S. because:
They are the leading cause of drug-related hospital admissions—often due to heart attacks, strokes, bleeding, and kidney failure.
Kidney damage is a significant risk.One study found a 20%increased risk of kidney disease from NSAIDs; others foundup to 212%. Amongst kidney failure patients,65.7% were found to be chronic NSAID users.
NSAIDs raise cardiovascular risks. NSAIDS also increase the risk of heart attacks and death (e.g., extensive studies have found between a 24-326% increase1,2,3). Two of the worst ones,Vioxx(Merck) andCelebrex(Pfizer), were designed to reduce stomach bleeding but instead caused heart attacks and strokes. Merck hid data on Vioxx's risks; eventually it was withdrawn after an estimated120,000 deaths. Celebrex, still on the market, has been linked to75,000 deaths. Merck’shandling of Vioxxlater informed how pharma pushed theHPV vaccineand mRNA vaccines.
Gastrointestinal bleeding is common and often fatal. In 1999,over 16,000 Americans died from it. NSAIDs also cause small bowel damagein over 50% of chronic users—often undetected—leading to"small bowel enteropathy"and possibly chronic illness through gut permeability.
They impair healing,especially of ligaments, creating long-term re-injury risk.
Trials alleging the benefit of NSAIDs are frequently intentionally deceptive and frequently create the illusion of a benefit where none exists. What this means is that many patients ruin their lives with drugsthat did almost nothing for them in the first place.—Peter Gøtzsche
Unfortunately, NSAIDs remain amongst the most commonly prescribed drugs, and are frequently given for musculoskeletal injuries.
Note: the dangers of NSAIDs are discussed furtherhere.
Tylenol
Tylenol (acetaminophen)is one of the few over-the-counter alternatives to NSAIDs and is generally consideredsafer, though oftenineffective for severe pain. Still, it carries serious risks:
Liver Toxicity: Overuse leads to56,000 ER visits, 2,600 hospitalizations, and 500 deaths annually in the U.S.due toTylenol toxicity.
Fever Suppression: Tylenol reduces fevers, which are key immune defenses. Suppressing them canworsen or prolong infections—a pattern observed duringCOVID-19. Many parents of vaccine-injured children reported symptoms (e.g., autism) appeared after using Tylenol to suppress high post-vaccine fevers, explored inthis 2021 paper.
**apentin and Pregabalin
**apentin (Neurontin) was originally approved to treat epilepsy—a small market. After approval, Pfizer aggressively pushed it for unapproved uses, especiallyneuropathic pain, despite limited evidence. The federal government fined Pfizer nearly $1 billion for illegal promotion.
While less toxic than NSAIDs, side effects for these drugs are common and include: lethargy, dizziness, sedation, and cognitive impairment, as well as rarer but serious reactions like respiratory depression and hypersensitivity. **apentin can also be habit forming.
Note: since **apentin and pregabalin (Lyrica) only work for specific types of pain (e.g., neuropathic pain), they typically do very little for most patients’ pain. However, they are widely prescribed because they lack many of the severe risks associated with other pain reducing drugs, and as a result, many are placed on inappropriate prescriptions for them.
Corticosteroids
Initially hailed as a wonder drug, corticosteroids like prednisone and hydrocortisone graduallywere discovered to have significant side effects(e.g., weight gain, adrenal suppression, heart attacks, diabetes, insomnia, and psychiatric effects). Since corticosteroids trigger tissue breakdown, they also often greatly weaken the body's structural integrity,impair wound healingand weaken collagen synthesis.
Furthermore, corticosteroids doubleone's risk of fracture(especially vertebrae), with12% of usersreporting fractures.Steroids cause 5-15% bone loss yearly, and37% of long-term users experience vertebral fractures. High dosesincrease vertebral fracture risk fivefold. Higher doses also cause avascular necrosis in6.7% of users. Likewise, they greatly impair wound healing, collagen
Note: the primary drugs used to treat Osteoporosis (bisphosphonates) have severe side effectshave severe side effectsincludingmaking the bones more likely to break. In turn, one of the few approved uses forbisphosphonatesis steroid-induced bone loss.
Since both collagen, ligaments (which are composed of collagen) and bones are weakened by steroids, chronic use leads to joint weakening and chronic pain. Because of this, we frequently encounter patients who achieved a temporary alleviation of joint pain (e.g., in the spine or knee) who then have their condition worsen and require surgery. Unfortunately, this side effect is rarely disclosed to patients, leading to many surgeries that could have been prevented.
Note: in many cases, if joint pain is instead treated by strengthening the ligaments (e.g., withnutritional supplementationorprolotherapy), the pain will resolve and future surgeries can be prevented.
The Surgery Funnel
Surgeries often have risks that patients don't learn about until after complications occur, which is problematic since you can't "undo" surgery. For this reason, patients should seek unbiased second opinions from doctors who aren’t being paid to do a proposed surgery.
Unbearable pain (e.g., in a joint) is one of the strongest motivators for surgery, and spinal surgeries are the most common elective surgery I'm consulted about. Unfortunately, since spinal surgeriesare one of the most profitable areas in medicine, there's reluctance to consider if risks outweigh benefits or ifsafer and more effective alternative exist, and over the years I’ve become increasingly skeptical of them, as while some are necessary and help patients, many are not.
Likewise, despite trillions spent on spinal pain (e.g., in 2016,134.4 billion dollars was spenton neck and low back pain in the USA), most patients remain stuck with chronic pain and experience significant side effects from treatments.
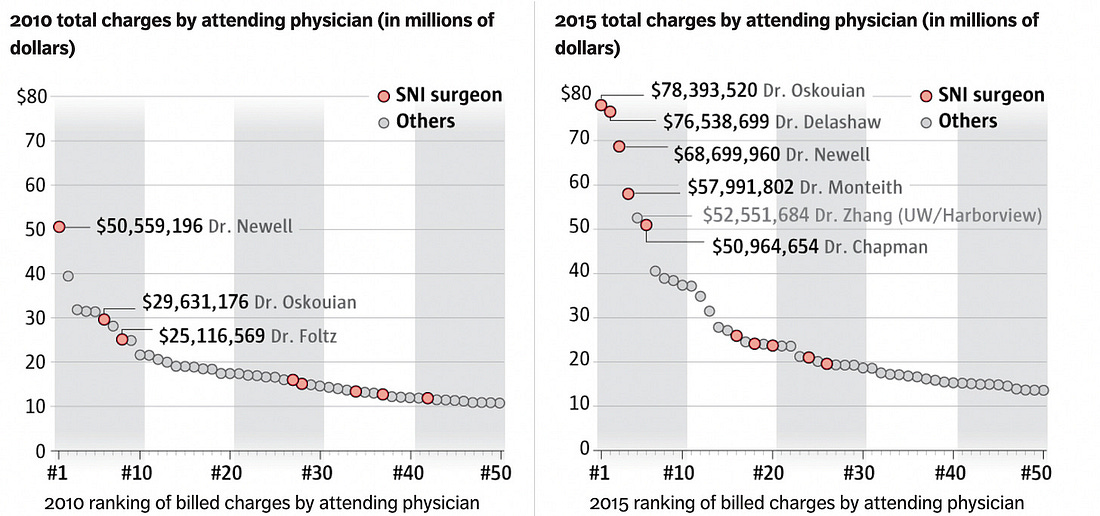
Note: there have beennumerous newspaper investigationsof spinal surgeons who recklessly performed large volumes of unnecessary surgeries, killing or injuring many of their patients who were nonetheless protected by their hospitals because of how much revenue they generated.
DMSO: A Safer Alternative
Over the last seven months, I have been working to spread awareness of dimethyl sulfoxide to the world, a natural compound which provides dramatic benefit for a variety of challenging conditions (e.g.,autoimmunity,strokes,paralysis,antibiotic resistant infections,cancers,vision lossand tinnitus).
DMSO also increases blood circulation to tissue, reduces inflammation, interrupts pain transmission, relaxes muscles, and decreases activity of the sympathetic nervous system. Because of this, DMSO is highly effective at:
•Healing tissue injury (includingparalyzing spinal cord injuries).
•Treating bursitis.
•Healing arthritis.
•Reducing acute and chronic pain.
•Treating many forms of pain, conventional therapies (including opioids) are often ineffective for such ascancer pain,complex regional pain syndrome,fibromyalgia,post-surgical painandphantom limb pain.For example, inthis article, I summarized dozens of studies (comprising thousands of patients) which consistently showed DMSO improved the majority of musculoskeletal conditions it was tested on (e.g.,one of 38 patientswith lumbar and disc herniations that found DMSO made them recover twice as quickly). Likewise, I have now receivedthousands of remarkable testimonialsfrom readers who used DMSO, most of which were of a significant improvement in pain or rapid healing of an injury.
Note: if you’ve had a DMSO experience you would like to share, please share ithereas once this series is finished, I will compile and summarize all your stories. Likewise, if you are presently using DMSO to treat patients and would like referrals, please let me know.In parallel, many doctors such as James Miller MD have been inspired to use in their practice and seen similar remarkable results for a variety of challenging conditions.
Note: in about 10-15% of people of people DMSO does not help their chronic pain. Typically this is either due to it being a chronic issue (where it can often take up to six weeks to get a response), too low of a dose being used, or the pain being psychiatric in nature (as from the earliest days of DMSO research,Merck noted that type of pain had a poorer response to DMSO).
For musculoskeletal injuries (e.g., pain or injuries), in most instances where a steroid or NSAID would be used, we find DMSO:
•Is more effective at addressing the immediate issues.
•Also heals the underlying issue (e.g., a herniated disc or injured ligament) rather than worsening it and creating future musculoskeletal injuries
•Does not have the myriad of (often severe) side effects frequently seen from standard treatment options.As such, for years, we’ve found that in most cases where drugs like NSAIDs are widely used, much better and far safer results could be obtained from DMSO. Unfortunately, while this was recognized in the past (e.g., many professional athletes in the 1960s and 1970s found DMSO dramatically improved their ability to recover from injuries and facilitated rapid returns to the field), all of that has now been largely forgotten. Consider for example, this 1980 60 Minutes episode:
Lastly one of DMSO’s key properties is that it can potentiate other substances and carry them inside the body (thereby making it possible to administer IV medications topically). As an almost infinite number of substances can be combined (e.g., I’m familiar with hundreds that have been successfully enhanced with DMSO combinations), this area still remains greatly understudied.
Of those that have been, most which have been approved by drug regulators around the world (e.g.,PENSSAID in the USA) combined DMSO with another substance recognized to have pain reducing characteristics (e.g., diclonfenac, capsicum, menthol, or hydroxyethyl salicylate). In many cases, these formulations enhance the pain reducing and tissue healing properties of DMSO.
Note: since there are so many different natural or pharmaceutical DMSO combination therapies, summarizing them has been the most challenging part of the DMSO series (and hence why it was the final part of the series and despite a lot of work, still is not quite done).Conclusion
The medical business model revolves around maximizing sales, either by perpetually selling a patient medications or by funneling them into high ticket items, and as I’ve tried to show here, pain management exemplifies this business model.
For instance, spinal surgeries (the last step for many patients whose pain was improperly managed), can make a hospital well over 100,000 each. In turn, asan investigation of numerous botched neurosurgeries showed, ambitious neurosurgeons (e.g., those who wanted to do so many surgeries they would often have multiple operating rooms running concurrently) will make enough money to sustain a hospital:
Similarly, as this article showed, patients with chronic pain are often put onto lifelong prescriptions of pain medications which fail to address much of their pain, have significant (and sometimes life-threatening) side effects, and frequently force them down the sales funnel to the lucrative joint and spine surgeries.
That predatory business model in turn, was exemplified by Purdue Pharma, whichbribed an FDA reviewerto claim their proprietary opioid (OxyContin) was not addictive. In 1995, the drug was then marketed with that claim and having theAmerican Pain Societydeclare “pain was the 5thvital sign,” compelling doctors to routinely assess for it and treat any existing pain with opioids (as otherwise they faced malpractice investigations from state medical boards). This, in turn, created the modern opioid crisis (as many opioid users develop permanent addictions after brief courses of these “non-addictive” drugs) which eventually affected so many communities doctors lost much of their ability to prescribe opioids to patients with crippling pain nothing else worked on.
In my eyes, the root cause of all of this is that since pain is an ideal market, there is very little interest in looking at either the shortcomings of existing treatments or looking into actual treatments for pain which destroy that perpetual revenue stream. Fortunately, the need to reduce wasteful spending (e.g., for costly and unnecessary surgery) MAHA moment is at last giving us a chance to change things and begin looking at the actual causes and treatments for these conditions rather than costly ones that do neither.
Author's note:This is an abridged version ofa longer articlethat goes into more detail on dangers of common pail killers like NSAIDs and safe alternatives for treating neck and spine pain (which can be readhere), along witha companion articleon how DMSO can treat pain injury and arthritis (which can be readhere), anarticle on the dangers of corticosteroids(which can be readhere) andan articleon the many dangers of spinal surgery (which can be readhere).
The Forgotten Side of Medicine is a reader-supported publication. To receive new posts and support my work, please consider becoming a free or paid subscriber.
Click below to share this post!
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewedhere. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewedhere.
You're currently a free subscriber toThe Forgotten Side of Medicine. For the full experience,upgrade your subscription.
LIKE
COMMENT
RESTACK
© 2025A Midwestern Doctor
Substack Inc., 111 Sutter St 7th Floor, San Francisco, United States 94104
Unsubscribe