Prospects for treating early stage COVID-19 remain uncertain, with a host of monoclonal antibody products and Starpharma’s (OTCQX:OTCQX:SPHRY) nasal SPL7013 antiviral spray vying for a role for prevention of infection and early treatment. Here I update on the latest developments with remdesivir, convalescent plasma, monoclonal antibodies and Starpharma’s SPL7013 antiviral. For investors, the stock to watch is Starpharma as over the last 3 trading days in Australia, the stock price on the ASX has risen almost 50% on good volume. With poor prospects for treatments for late stage COVID disease, and anyone’s guess whether there will be an effective vaccine and in what time frame, effective early treatment/prevention is of considerable interest. Otherwise it is just social distancing, masks, lots of testing and (when the case load is low enough) lots of contact tracing, with economies sliding in and out of lockdown. Remdesivir treatment range narrows
In early June I wrote an article indicating that Gilead’s (NASDAQ:GILD) antiviral remdesivir might be as good as it gets for treating COVID-19. Since then Dexamethasone has become the only treatment with clear life-saving capacity, albeit only for patients with end stage disease. The utility of Dexamethasone significantly locks remdesivir out of the end stage treatment space. Remdesivir is getting a lot of attention as after Dexamethasone it has attracted most attention for treating COVID-19, and its effect is largely for serious (mostly requiring oxygen) but not yet life-threatening disease. Recently results were released concerning possible use of remdesivir at an earlier stage, although still with hospitalised patients that had moderate COVID-19 pneumonia. 584 patients with moderate COVID-19 were examined in a Phase 3 trial. The patients had a mean age of 57 and 56% had cardiovascular disease, 42% hypertension, 40% diabetes and 14% asthma, indicating a group with a propensity towards serious COVID-19 outcomes. Those patients involving a 5 day remdesivir treatment performed significantly better than standard care, but surprisingly those on an 11 day treatment protocol showed no significant benefit. The conclusion from this trial is that remdesivir has an uncertain clinical value for these earlier stage patients. This might mean that remdesivir might have a rather narrow treatment profile. One feature of the study was that it is not easy to predict who will progress to life-threatening disease. The study was open label and this could have meant that since it was known how each patient was being treated, this may have had some impact on the way they were treated.
Overall the trial seeking to extend the range of remdesivir treatment to earlier stage disease seems inconclusive. Convalescent plasma becomes political, but does it work?
Convalescent plasma is an obvious, if limited, possible treatment option for COVID-19 and more than 70,000 US patients have received treatment. A preprint on the medRxiv server details analysis of 35,322 really sick patients from the US and its territories who received convalescent plasma transfusions. This study gives some grounds for suspecting that convalescent plasma might become part of the treatment landscape. There was an indication of improvement (in both 7 and 30-day mortality) with patients who received higher levels of antibody in the convalescent plasma. So the results are encouraging, although the degree of the response was quite small (7 day death rate for low antibodies was 13.7%, while high antibodies produced 8.9% mortality). The scientific report indicated that this data will be useful in designing randomised clinical trials to see if convalescent could be a useful treatment. Note that no placebo controlled clinical trials have yet been conducted, so it could still be the case that convalescent plasma is not an effective treatment.
The above report was so far so good, and then President Trump made the following statement with reference to convalescent plasma at a White House briefing : “Today I am pleased to make a truly historic announcement in our battle against the China virus that will save countless lives. Today’s action will dramatically increase access to this treatment.”
He was referring to the FDA having approved Emergency Use Application (EUA) of convalescent plasma. This was surprising as two key health scientists, National Institutes of Health Director Dr Francis Collins and the Director of the National Institute of Allergy and Infectious Diseases Dr Anthony Fauci saw it differently and had earlier intervened in a plan by the FDA to release an EUA for convalescent plasma, because the data was too weak to justify such authorisation.
The FDA Commissioner Stephen Hahn in a press conference with President Trump supported the President’s view that the results with convalescent plasma were remarkable, saving 35 out of 100 lives of people who were treated with the convalescent plasma. In fact the results did not show this and Hahn apologised for the error.
The jury is out as to whether convalescent plasma will be an effective treatment, pending placebo controlled trials. Monoclonal antibody treatments
A tidal wave of monoclonal antibody treatments is coming.
The idea of using specific monoclonal antibodies or cocktails of them provides a standardised and scalable product, unlike the situation with convalescent plasma, which is a variable product in limited supply. The Syrian golden hamster has been used as an animal model to screen for protective monoclonal antibodies that bind to SARS-CoV-19.
Monoclonal antibodies need to be injected, which makes them less accessible than a nasal spray (which addresses a major site of initial infection by SARS-CoV-2). The most interesting aspect of monoclonal antibody approaches is whether they can offer relatively long term protection.
AstraZeneca’s (NYSE:AZN) AZD7442 is a combination of 2 monoclonal antibodies which resulted from a study of convalescent serum of COVID-19 patients. AstraZeneca’s twist is to modify the antibodies, especially hoping to give them a longer life when injected. The hope is that AZD7442 might be effective for up to 6 months. This could be very interesting if it pans out. A 48 patient Phase 1 trial was commenced this week.
Regeneron (NASDAQ:REGN) and Roche (OTCQX:OTCQX:RHHBY) are collaborating on another dual monoclonal antibody (REGN-COV2) treatment for early stage COVID-19 and possibly as a preventative. There are 2 Phase 2/3 trials investigating treatment of COVID-19, and a Phase 3 trial for preventing COVID-19 in contacts of infected individuals. Regeneron will distribute the product (if successful) in the US and Roche will distribute in the rest of the world, with Roche securing EMA (European Medicines Agency) approval and any other approvals needed outside of the US.
Eli Lilly (NYSE:LLY) has started a Phase 3 BLAZE-2 trial of its monoclonal antibody LY-CoV555 with a focus on nursing home residents and staff. LY-CoV555 is administered intravenously. Clearly a product that was effective in nursing homes could be very interesting because of the huge problems in nursing home worldwide.
Time will tell how monoclonal antibody treatments will be received as they require injection. How long lasting they will be is unclear, although AstraZeneca is making some bold claims about likely longevity of its AZD7442 dual monoclonal antibody combination. Starpharma’s SPL7013 antiviral is not going away
Leaving the best investment opportunity until last, here I update earlier articles on May 4 and on August 6 concerning Starpharma’s plans to repurpose its antiviral SPL7013 for early stage COVID treatment and prevention of infection. Two days ago Starpharma provided an update indicating significant progress in repurposing SPL7013 for COVID treatment.
Firstly, formulations of SPL7013 have been developed as a nasal spray, a manufacturer selected and pilot manufacture is underway. The final formulation will have an activity several thousand fold higher than that which has antiviral action on SARS-CoV-2.
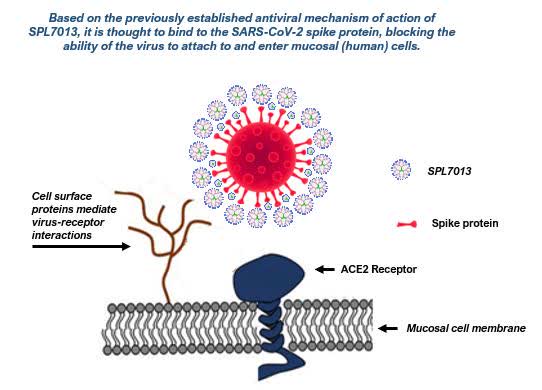
Additional work has been done on the mode of action (blocking viral attachment to human mucosal cells) and a publication submitted. This publication is worth reading for a comparison with the antiviral action of remdesivir (much weaker) and for details about mechanism of action. SPL7013 is not systemically absorbed so it is well suited to act as a preventative as well as having antiviral properties.
Source Starpharma The red sphere with spikes is the SARS-CoV-2 virus
Starpharma has compiled regulatory documentation and an expedited regulatory pathway has been confirmed for important markets including Europe. Regulators indicate that approval of the nasal spray formulation can be expedited by leveraging non-clinical and clinical data for marketed products containing the active ingredient SPL7013.
Starpharma CEO Jackie Fairley made the following comments about the positioning of SPL7013 for COVID prevention and treatment: “The SPL7013 nasal spray has the potential to complement vaccine strategies to further reduce risk by preventing acquisition and transmission of SARS-CoV-2, and reducing disease progression due to ongoing viral replication in mild forms of COVID-19. Feedback from infectious disease specialists and other healthcare agencies has confirmed that a cost-effective and readily available product to help prevent SARS-CoV-2 infection would be highly valued and play an important role in reducing transmission for the broader population and especially for frontline workers in the health, aged care and travel industries.
Whilst the initial focus is on a nasal spray as the most rapid path to market, …SPL7013 could be applied via other routes of administration, such as ocular, nebulised or injection.
The SPL7013 active is patented by Starpharma in major markets, and a specific patent application has been filed for the COVID-19 nasal spray. Starpharma has also commenced confidential commercialisation discussions, having shared product details and supporting technical data with a number of interested pharmaceutical companies, covering a range of geographic markets.”
It will be interesting to see how the monoclonal antibody products compare with Starpharma’s SPL7013 antiviral on effectiveness and price. Conclusion
Viruses are tough nuts to crack and the COVID-19 pandemic emphasises this point. You can be certain that just about every drug ever developed has been considered as a possible repurposing opportunity to treat COVID-19, yet the pickings are still slim for COVID-19 treatments. The dark horses are a host of monoclonal antibodies targeting the virus and Starpharma’s SPL7013 antiviral, all of which have potential for early stage treatment and possibly as preventatives. Starpharma’s SPL7013 is attractive because it is being formulated as a nasal spray, while the monoclonal antibodies are injected.
In terms of interest to investors, Gilead’s remdesivir is looking to be less effective than initial euphoria indicated. It isn’t yet clear what size the market will end up being for remdesivir as the treatment window is starting to look narrow.
Convalescent plasma is becoming political, as happened with the hydroxychloroquine story. Hydroxychloroquine/chloroquine have been clearly shown to be ineffective now. While there are reasons to suspect that convalescent plasma might work, this is not yet proven. Anyway it is hard to productise convalescent plasma, so it would be a niche product at best. Monoclonal antibodies offer better prospects as treatments for COVID-19.
Every big pharma company (and lots of smaller biotech companies) has a portfolio of monoclonal antibodies which might have application, including a range of monoclonal antibodies that specifically target the SARS-CoV-2 virus, and it is clear that there is a lot of innovation about building effective products for early stage treatment and as possible preventatives. It is too soon to know how the monoclonal antibody products will perform, and mostly they belong to large companies who are probably too big to have these products impact their share price significantly, although I could be wrong about this.
Starpharma’s antiviral SPL7013 is different because it shows interesting activity and the active ingredient is being marketed for other applications in a number of countries, except the US where FDA approval is on a slow train. Starpharma is a small company that has interesting prospects but it has been largely ignored. The latest announcement about progress with formulating SPL7013 for early stage treatment and prevention of COVID-19 has produced action, with the stock up in Australia from $A1.05 on 25th August to $A1.47 at today’s (27th August) close. There is potential for more as the stock is only back to trading at its year high. It looks like there will be rapid progress in Europe on the COVID-19 early treatment/prevention, so watch this space.
Starpharma’s COVID-19 treatment opportunity is not all that this company has going for it. As I’ve indicated in several articles, this is a hidden gem worthy of consideration at the risky end of one’s portfolio.
I am not a financial advisor, but I have a background in biotech both from a technical and also investor perspective. If my commentary helps you and your financial advisor to think about whether you want to invest companies offering COVID-19 treatments, please consider following me. I am a long time investor in Starpharma, so please take note of that in my discussion about SPL7013.
Disclosure: I am/we are long SPHRY. I wrote this article myself, and it expresses my own opinions. I am not receiving compensation for it (other than from Seeking Alpha). I have no business relationship with any company whose stock is mentioned in this article.
SPL Price at posting:
$1.47 Sentiment: Buy Disclosure: Held










 (20min delay)
(20min delay)